Advanced pharmaceutical bulletin. 15(3):574-587.
doi: 10.34172/apb.025.45384
Mini Review
Decrypting the Potential of Lipidic Vesicular System for Delivery Enhancement of Tranexamic Acid in Melasma Hyperpigmentation Treatment
Xin Lu Soo Conceptualization, Data curation, Funding acquisition, Project administration, Visualization, Writing – original draft, Writing – review & editing, 1 
Kang Nien How Conceptualization, Supervision, Validation, Writing – review & editing, 2, 3
Zee Wei Lai Conceptualization, Supervision, Validation, Writing – review & editing, 1, *
Author information:
1School of Biosciences, Taylor’s University Lakeside Campus, 47500 Subang Jaya, Malaysia
2Dermatology Unit, Department of Medicine, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia, Serdang 43400, Malaysia
3Dermatology Unit, Hospital Sultan Abdul Aziz Shah, Universiti Putra Malaysia, Serdang 43400, Malaysia
Abstract
Melasma is a prevalent pigmentary disorder characterized by irregular brown patches on sun-exposed face and neck regions, driven by increased vascular proliferation and dysregulated melanogenesis. Although benign, untreated melasma significantly impacts quality of life from emotional stress and cosmetic impairment especially for Asian women. Melasma complex and diverse aetiology involves melanocyte hyperactivity triggered by UVR exposure, genetics, hormones and aging. The effectiveness of current topical and physical therapies such as depigmenting agents, peels, photoablation and dermabrasion etc. have varying efficacy but limited by high recurrence rates. Tranexamic acid (TA) is a lysine-derived antifibrinolytic drug which has demonstrated high potential in reduction of melanogenic factors, inhibiting melanogenesis. Lipidic vesicular delivery systems including liposomes, ethosomes, niosomes, transferosomes and phytosomes showed extensive capability in the delivery of TA into deeper epidermal layers with improved stability and penetration efficacy. Multiple studies have shown that lipidic vesicular formulations of TA offer improved safety and efficacy compared to conventional delivery methods. However, further research and clinical trials will be necessary to verify the long-term safety and feasibility and to set up standardized protocols for this novel delivery system. Therefore, this review aims to scrutinize the potential of lipidic vesicles as a cutting-edge novel approach for the enhancement of TA’s efficacy in melasma hyperpigmentation treatment, as well as offering possibilities for future research and clinical applications in dermatology.
Keywords: Drug delivery, Hyperpigmentation, Lipidic vesicular, Melasma, Nanotechnology, Skin barrier, Tranexamic acid
Copyright and License Information
© 2025 The Author (s).
This is an Open Access article distributed under the terms of the Creative Commons Attribution (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, as long as the original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
This study was supported by the funding provided to Xin Lu Soo through Full-Time Graduate Research Assistant (GRA) positions at the School of Biosciences, Taylor’s University under the Taylor’s Research Excellence Scholarship, which fully covered her tuition fees.
Introduction
Skin hyperpigmentation disorders particularly melasma is a highly prevalent pigmentary condition characterized by enhanced vascularization and disrupted melanogenesis in human skin. The most frequent melasma’s characteristic is the irregular appearance of contrast brown patches on the face or neck especially at sites of frequent solar exposure.1 Although melasma is medically benign, untreated cases can significantly impair life quality due to cosmetic concerns and associated psychological distress.2 Melasma affects all ethnicities with Asian women of reproductive age and darker skin phototypes accounting for up to 90% of cases.3,4 This condition develops when hyperactive melanocytes increase melanin synthesis and deposit excess pigment in the skin epidermis. Nevertheless, its pathogenesis is multifactorial including ultraviolet radiation (UVR), genetic predisposition, hormonal influences and aging.5,6
Current melasma therapeutic approaches include topical depigmenting agents and procedural interventions but remain limited by high relapse and recurrence rates.7,8 Hydroquinone and retinoids are the most frequently prescribed topical depigmenting agents. The “New Trio” therapy cream containing isobutyl amide-thiazolyl-resorcinol, retinoic acid and dexamethasone have demonstrated comparable efficacy and tolerability to the gold-standard “Kligman’s Trio” comprising hydroquinone, tretinoin and corticosteroid in reducing Melasma Area and Severity Index (MASI) score by approximately 50% after 8-12 weeks of use.9,10 Furthermore, procedural treatments including laser therapy, microneedling, dermabrasion and acid-based chemical peels serve as secondary options. Combination treatments such as hydroquinone with laser therapy have shown more durable melanogenesis suppression than monotherapy.8,11 However, treatment effects remain inconsistent and adverse effects including post-inflammatory hyperpigmentation, erythema and barrier disruption compromise overall success. As a result, the pursuit for a safer, more effective and innovative therapeutic strategy for melasma remains an active area of research.
Tranexamic acid (TA) has recently gained recognition as a promising therapeutic agent for melasma. Its’ first documented dermatological application was in 1979 by Sadako from Japan who observed a significant reduction in melasma severity within 2 weeks.12 TA is a synthetic lysine analogue with antifibrinolytic activity that hinders paracrine melanogenic mediators which induce melanocytes synthesis and has historically been used to prevent haemorrhagic episodes.13 Furthermore, TA competitively binds to the lysine-site of plasminogen, thereby inhibiting its conversion to plasmin and stabilizing the fibrin matrix. Additionally, TA directly inhibits tyrosinase activity thereby downregulating melanogenesis and reducing hyperpigmentation.14 Researchers have studied TA in topical, oral, intradermal and microneedle-assisted formulations reporting measurable reductions in pigmentation indices and improvements in patient satisfaction scores as a skin-lightening agent. Meta-analyses confirm that oral TA effectively reduces melasma pigmentation and is additionally beneficial in other skin diseases like eczema.15-19 Oral TA increases cutaneous vascularity and mast-cell density while attenuating epidermal hyperpigmentation.18,20 However, extensive oral administration may lead to multiple side effects like headaches, menstrual irregularities, gastrointestinal disturbances and rare thromboembolic events.21-23 On the other hand, OTC topical TA gels, creams and solutions have demonstrated favourable safety profiles.24,25 Multiple studies reported that topical TA yields moderate to marked pigment reduction with lesser systemic adverse effects compared with oral therapy.26,27
Nevertheless, topical TA suffers from poor epidermal penetration and retention which severely compromises therapeutic efficacy.16,28 This is mainly due to its hydrophilic and zwitterionic structure causes repulsion by the lipophilic stratum corneum (SC) barrier, preventing adequate delivery to melanocyte-rich basal epidermis. Moreover, rapid systemic absorption reduces epidermal residence time which further attenuate its melanogenic impact.29-31 Consequently, topical TA treatment durations exceeding 3 months are often required to achieve visible improvement with recurrence frequently observed.18 To overcome these limitations, several methods especially the nanostructured delivery systems including lipidic vesicular system and polymeric based have been explored to enhance TA skin penetration.32 Among these, lipidic vesicular systems are especially promising due to their unique physicochemical features where their bilayer structure simultaneously solubilizes hydrophilic drugs and fuses with SC lipids, thereby improving drug deposition while maintaining safety. This review article therefore focused on exploring the novel concept of lipidic vesicular delivery system as a rational solution to the delivery limitations of topical TA, improving its efficacy and safety for melasma management.
Melasma and hyperpigmentation
Overview of melasma and hyperpigmentation
Melanogenesis is a complex biological process occurring within the melanocytes where melanin, the pigment responsible for photoprotection and integumentary coloration is produced. However, excessive melanin production by hyperactive melanocytes can lead to pigmentation disorders including melasma. Melasma is a common cosmetic ailment that can be identified by symmetrically distributed brownish facial patches and décolletage which worsen with extreme sun exposure.3,6 It has been categorized into three histologic variants: epidermal, dermal, and mixed which is distinguishable through Wood’s lamp examination and visible light assessment. The epidermal type is marked by increased melanin deposition across the epidermis, accompanied by enlarged melanocytes and a higher density of melanosomes. The dermal type is defined by the presence of melanophages in both the superficial and deep dermis whereas the mixed type exhibits histopathological characteristics of both epidermal and dermal patterns.16,28 The Melasma Area and Severity Index (MASI) score is the commonly used and validated tool for evaluating melasma severity and therapeutic outcomes.33 Although the precise pathogenesis remains unclear, multiple factors have been identified to aggravate melasma onset including UVR, genetic predisposition, hormonal dysregulation and medications shown in Figure 1.34
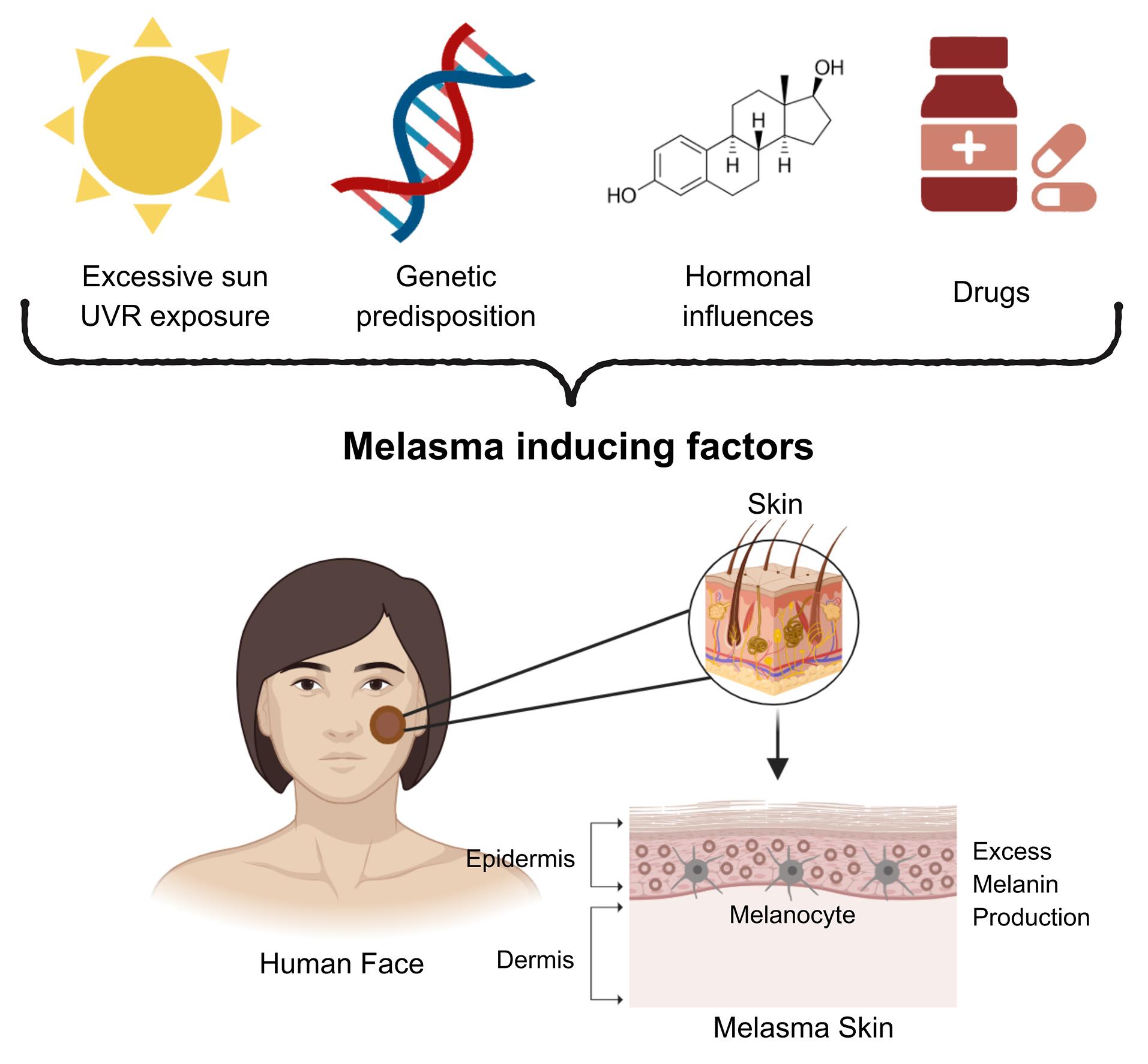
Figure 1.
Key contributing factors of melasma: excessive sun UVR exposure, genetic predisposition, hormonal influences and drugs
.
Key contributing factors of melasma: excessive sun UVR exposure, genetic predisposition, hormonal influences and drugs
Pathogenesis of melasma and hyperpigmentation
Numerous pathological explanations have been made in which UVR from sun exposure being the primary inducer of melanogenesis and melanosome transfer, triggering tyrosinase activity and leading to pigmentation as well as contributing to skin photoaging. Recent studies have confirmed the strong association between UVR and melasma development. Alcantara et al35 observed increased epidermal melanogenic response in both melasma-affected and adjacent normal skin after UVR exposure, regardless of extended exposure with photoprotection or brief uncontrolled exposure. Similarly, Sarkar et al36 reported that more than 50% of male melasma patients in their study were outdoor labourers and nearly 30% resided in mountainous regions with high sun exposure. These findings establish UVR as the major contributing factor to melasma development as it selectively darkens affected areas more than normal skin. UVR can activate melanocytes by inducing keratinocytes, fibroblasts and endothelial cells to secrete paracrine mediators that upregulate melanogenesis.5,32,37 The melanogenesis mechanism triggered by UVR is illustrated in Figure 2.
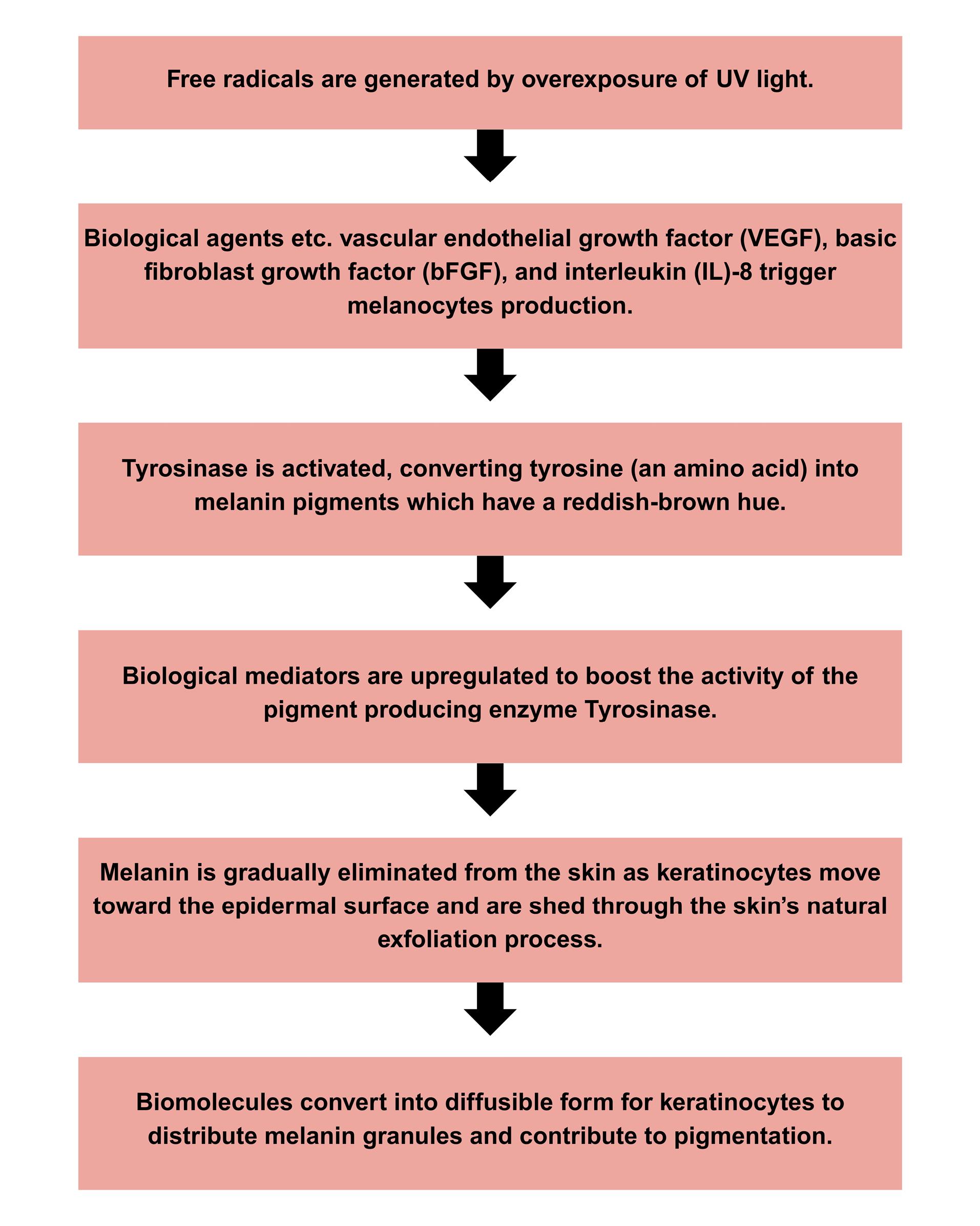
Figure 2.
UV-induced pathway of melanin biosynthesis
.
UV-induced pathway of melanin biosynthesis
Additionally, melasma involves dysregulation of more than 150 genes associated with both immediate and long-term modulation of pigmentation pathways. An individual’s inherent melanocyte count which governs melanin synthesis and skin colour is primarily determined by their genetic makeup.38 Significant ethnic variability in melasma prevalence has been observed, with familial clustering further implicating genetic predisposition as a major risk factor.39 These findings were in accordance with a multinational study by Ortonne et al40 involving 324 women where they reported 48% of the subjects exhibited a family history of melasma with 97% restricted to immediate relatives. Similarly, Tamega et al41 reported a familial history in 56% of 302 Brazilian patients involving identical twin sisters’ cases, supporting the genetic foundation of the condition. Facial melasma has been hypothesized to be inherited in a dominant fashion with environmental factors triggering onset in genetically susceptible individuals.42 Furthermore, darker skin individuals tend to have higher level of basal melanin and larger melanosomes which may further increase susceptibility.43
Hormonal factors also contribute in melasma pathophysiology particularly oestrogen suggesting an increased risk in pregnant women, post-pubertal females and oral contraceptive users.44 Epidemiological studies suggest wide variability in hormone-related melasma prevalence across populations. For instance, Tamega et al41 reported that 36.4% of subjects in a Brazilian cohort experienced melasma onset during pregnancy, while 16.2% was caused by oral contraceptive use. Similarly, a cross-sectional study conducted in Indonesia revealed a melasma prevalence of 91.7% among 36 women taking oral contraceptives, demonstrating a positive correlation between incidence and usage duration.45 Elevated expression of oestrogen receptors (ER) and progesterone receptors (PR) has been consistently observed in melasma-affected dermal tissues at the molecular level.46-48 Upon binding to ERs, oestrogen activates rate-limiting tyrosinase in melanogenesis, thereby enhancing synthesis of melanin. Moreover, the upregulation of ion-exchange regulatory protein PDZ domain-containing kidney 1 (PDZK1) in melasma lesions has been found to potentially facilitating interactions between oestrogen signalling and ion transport mechanisms that promote melanogenesis and melanosome transfer.39,49,50 It was also postulated that oestrogen contributed to keratinocyte growth factor (KGF) production which affects melanocyte proliferation, tyrosinase activity and melanosome transfer ultimately resulting in melasma.34,51
Tranexamic acid (TA)
Overview of TA
TA is a haemostatic agent conventionally used since 1979 for the clinical management of irregular bleeding then repurposed for skin hyperpigmentation treatment.12,52 As a promising depigmentation agent, TA offers a viable topical treatment option for melasma individuals across varying degrees of severity. TA exhibits superior physicochemical stability with an oxidation half-life exceeding 24 hours at 40 °C as compared to other depigmentation agents such as arbutin, ascorbic acid, azelaic acid and glycolic acid which display variable stability and inconsistent success rates in melasma management.53-54 In a randomized controlled trial by Atefi et al,26 topical TA demonstrated non-inferiority to 5% hydroquinone achieving a mMASI score reduction to 2.30 as compared with HQ (P = 0.850) with a similar result reported by Sandeep et al55 Furthermore, direct comparisons with arbutin which is another standard agent remain limited but available data suggest TA achieves numerically greater MASI reductions (6.2 vs 3.4) without reaching statistical significance in small cohorts. Mechanistically, TA functions as a plasmin inhibitor thereby reducing the production of inflammatory mediators essential for melanogenesis.56 It can be administered via topical (2%-5%), intravenous intradermal (4 mg/mL) and oral dosing (500-1000 mg daily) with combination therapy often employed to enhance depigmentation efficacy.49 However, long term oral administration specifically more than 6 months is associated with a 2-4 % incidence of gastrointestinal disturbance and < 0.1% absolute risk of thromboembolic events. In contrast, topical or intradermal TA is associated with mild, transient erythema or irritation ( < 15% incidence) and no reported vascular events.18,21
Mechanism of TA in melasma hyperpigmentation
The precise mechanism by which TA attenuates melasma hyperpigmentation remains under investigation. Limited studies suggest that TA primarily acts through suppression of plasmin activity, thereby disrupting melanocyte activation and melanin synthesis. TA inhibits plasminogen’s lysine-binding sites, effectively suppressing its conversion to plasmin and subsequently downregulating melanocyte-keratinocyte interactions that drive melanogenesis.57 Maeda and Tomita58 demonstrated that TA impedes melanocytes’ melanin synthesis by blocking the plasminogen-plasmin pathway and preventing melanocyte-keratinocyte interaction. Similarly, Maeda and Naganuma59 reported that TA reduced melanocyte tyrosinase activity in UVR-induced hyperpigmentation guinea pigs by preventing plasminogen binding to keratinocytes. Additionally, TA may suppress melanogenesis by inhibiting plasminogen-keratinocyte interaction which reduce prostaglandin and free arachidonic acid synthesis as well as tyrosinase activity. These findings were supported by a split-face study involving 40 melasma patients.60 Renckens et al61 suggested that TA inhibits plasmin activity on fibrin and cells by competitively interacting to plasminogen’s high-affinity lysine sites. Thus, it prevents the surface-mediated conversion of plasminogen to plasmin.
Beyond melanocyte regulation, plasmin is also crucial in angiogenesis. Plasmin-mediated degradation of extracellular matrix-bound vascular endothelial growth factor (VEGF) generates diffusible VEGF forms that promote neovascularization. As a plasmin inhibitor, TA ceases basic fibroblast growth factor (bFGF)-induced angiogenesis, thereby indirectly reducing pigmentation.62-63 Zhu et al1 reported that TA significantly inhibited tyrosinase activity, melanin synthesis and VEGF-induced melanogenic protein expression when VEGF receptors were neutralized. Similarly, in a clinical study involving 25 melasma women, topical TA demonstrated its ability to suppress bFGF and VEGF-mediated angiogenesis, resulting in decreased melanogenesis.20 Additionally, TA exhibits structural resemblance to tyrosine, enabling competitive inhibition of tyrosinase which further enhance its depigmentation efficacy.14,15 Although the exact molecular pathways remain incompletely defined, current evidence suggests that TA exerts its anti-melanogenic effects through two mechanisms: (i) plasmin inhibition which disrupts inflammatory and angiogenic pathways, and (ii) direct enzymatic inhibition of tyrosinase. Collectively, these mechanisms contribute to the clinical efficacy of TA in reducing melasma pigmentation across diverse patient populations.
Pharmacologic of TA for melasma hyperpigmentation treatment
Pharmacological therapy of TA for melasma involves oral or topical administration. Oral administration remains the most conventional approach with multiple clinical trials confirming its efficacy in managing melasma-related hyperpigmentation. A placebo-controlled randomized study administering 250 mg of TA twice daily for 3 months to patients with moderate-to-severe melasma demonstrated significant improvements particularly in severe cases but effects were not sustained post-treatment.18 Furthermore, Bhattacharjee et al64 further compared TA administered at 250 mg and 500 mg two times per day, observing equivalent therapeutic outcomes with no notable differences in tolerability. Similarly, Wang et al14 assessed 250 mg TA administered twice versus thrice daily over 12 weeks, revealing comparable therapeutic outcomes. A prospective clinical trial examined oral TA dosages from 500 to 1500 mg/d over treatment periods from one month to two years, finding progressive MASI score reductions across all groups with no significant differences between doses.65 These findings indicate that oral TA is effective starting at 250 mg, with therapeutic effectiveness more dependent on duration than dosage. However, prolonged use may reduce adherence due to common side effects such as gastrointestinal damages and menstrual irregularities.18,21-23
In addition to the oral administration route, TA has demonstrated skin-lightening effects when applied topically at concentrations between 2-5%.20,32 In a study by Yoo et al27 reported substantial melasma improvement over 10 weeks with a TA-containing cream, finding MASI score reduction and high patient satisfaction. Another trial showed that 2% TA cream reduced hyperpigmentation in mild melasma patients with no adverse effects observed after three months.24 According to Fox’s25 clinical study, 80% of subjects experienced significant melasma improvement after using a TA emulsion for 6 months with no adverse effects. Similarly, a comparative trial between 5% TA solution to a 2% hydroquinone (HQ) solution in 60 women with epidermal melasma found TA particularly effective. The TA group reported a 33.3% satisfaction rate which is greater than 6.7% observed from HQ group, attributed to faster visible effects and minimal side effects.26 These findings suggest that topical TA can effectively reduce melasma severity, although its onset of action may be slower than oral administration. Therefore, further research is required to optimize topical TA formulations for improved skin penetration and to accelerate visible clinical results.
Novel lipidic vesicular approach in TA delivery
Overview of lipidic vesicular system
Lipidic vesicular systems have gained significant attention in cell membrane biology emerging as a promising approach for trans-epidermal drug administration.66 Their ability to facilitate delivery of encapsulated drugs while acting as a depot system enhances stratum corneum (SC) penetration and facilitates continuous drug release by acting as a membrane barrier that controls skin absorption rates.67-69 Lipidic vesicles are organized spherical structures containing single or multiple concentric bilayers, formed through amphiphilic molecules’ self-assembly in water.70 Various types of lipidic vesicular drug delivery systems such as liposomes, ethosomes, niosomes, transfersomes and phytosomes have been developed for the delivery enhancement of depigmenting agents and TA to improve melasma hyperpigmentation treatment (Table 1). Figure 3 provides a schematic illustration of various vesicle structural organizations.
Table 1.
Various lipidic vesicular carriers with their advantages and drawbacks
|
Lipidic carriers
|
Characteristics
|
Advantages
|
Disadvantages
|
Ref.
|
| Liposomes |
simple
-
- Composed of phospholipids and cholesterol
-
- Amphiphilic hollow lipid bilayer sphere
|
simple
-
- Able to encapsulate both hydrophobic and hydrophilic drug molecules
-
- Non-toxic and biodegradable
|
simple
-
-
- Susceptible to oxidation and degradation
-
- High manufacturing cost
|
71-74
|
| Ethosomes |
simple
-
- Composed of 20-45% ethanol, phosphatidylcholine, cholesterol and water
|
simple
-
-
- Superior skin penetration and systemic circulation
|
simple
-
- May cause skin irritation if ethanol content exceeds 30%
-
- Solubility and compatibility issues for certain drugs
|
75-77
|
| Niosomes |
simple
-
- Single or multilamellar
-
- Developed from non-ionic surfactants in combination with cholesterol
|
simple
-
- More stable and lower formulation cost than liposomes
-
- Non-ionic surfactants enhance vesicle stability
|
simple
-
- Time consuming process for manufacturing
-
- Limited long-term in vivo safety data
-
- Potential surfactant toxicity
|
66,78-80
|
| Transferosomes |
simple
-
-
- Aqueous core encapsulated within a phospholipid bilayer with edge activator
|
simple
-
- Highly elastic and deformable
-
- Effective for large and hydrophilic molecules
|
simple
-
- Difficulty in encapsulating hydrophobic drugs
-
- Complex physicochemical optimization needed
|
66-67,81-82
|
| Phytosomes |
simple
-
- Molecular complexes formed between phospholipids and polyphenols
|
simple
-
-
- Synergistic enhancement of bioactive compound delivery and therapeutic efficacy.
|
simple
-
- Reduce concentration of active ingredient due to dependency on plant material
-
- Limited clinical data for safety and efficacy
|
83-84
|
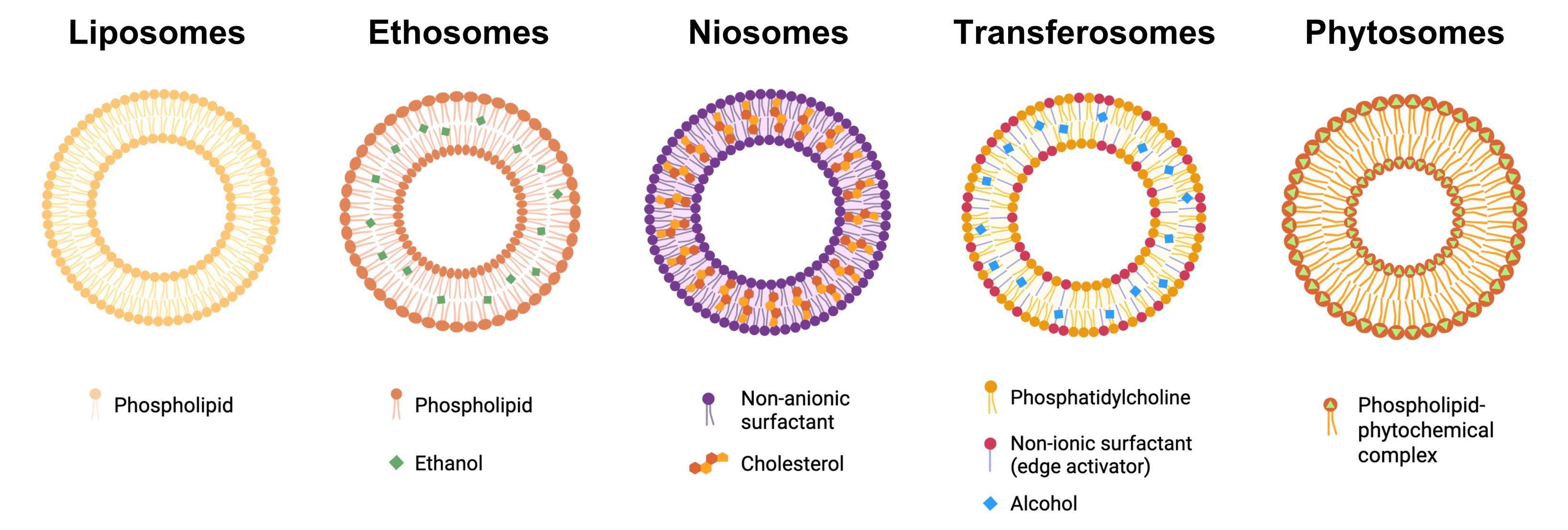
Figure 3.
Schematic representation of lipidic vesicular systems including liposomes, ethosomes, niosomes, transferosomes and phytosomes
.
Schematic representation of lipidic vesicular systems including liposomes, ethosomes, niosomes, transferosomes and phytosomes
Liposomes
Liposomes were initially used in membrane research in 1965 and were later proposed as drug delivery systems in 1972.71 Conventional liposomes primarily composed of phospholipids and cholesterol. Amphiphilic phospholipids with polar heads and nonpolar tails are the main building blocks of liposomes which enable them to encapsulate both water and lipid soluble substances.72 Consequently, liposomes represent a significant advancement in drug and cosmetic delivery by enhancing stability, possessing high biocompatibility and low toxicity. Empty liposomes exhibited 100% cell viability, while drug-loaded liposomes maintained over 50% cell viability following 24 hours exposure at a 5.37 µg/mL concentration in Vero cell line cultures derived from monkey kidney. The observed cytotoxicity was found to be concentration-dependent, with increasing drug concentrations corresponding to a higher percentage of cell growth inhibition.85 This finding aligns with Nguyen et al86 observations who suggested that increased cytotoxicity associated with liposomal formulations may result from enhanced cellular uptake.
According to studies, liposomes also enable targeted drug delivery and improved pharmacokinetics.66,87 Liposomes enhance drug delivery by fusing with cell membranes and disrupting SC lipid organization, thereby facilitating transdermal penetration.68,87 Additionally, factors such as drug molecule size, oil-water distribution coefficient and lipid membranes interactions can influence delivery efficiency within liposomes.72 Studies by Kirjavainen et al88 and Maghraby, Williams, and Barry89 suggested that liposomes promote drug absorption by modifying the skin’s outermost layer, thereby enabling increased pharmaceutical uptake and enhance skin penetration. However, liposomes clinical application may be limited by high production costs with expenses exceeding over US$ 1000 per gram of active pharmaceutical ingredient and requiring cold-chain storage which further increases logistical complexity and cost.73-74
Liposome have been widely utilized for various drugs notably for TA, where the presence of lipids within liposomes may reduce irritation and provide long-lasting moisturizing benefits.90,91 TA is incorporated within the aqueous phase of liposomes due to its hydrophilic nature. According to studies, it was hypothesized that liposomes enhanced TA percutaneous transport through merging the phospholipid bilayer with intercellular lipid to create transient hydrophilic channels that circumvent the intact SC and improved drug accumulation in follicular openings.92,93 Liposomes have demonstrated effective transdermal delivery of TA using various lipid compositions with diverse surface charges, including hydrogenated soya phosphatidylcholine, cholesterol, stearyl amine and dicetyl-phosphate.94 Moreover, TA-entrapped liposomes exhibit enhanced physical stability, high drug entrapment efficiency ( > 90% for up to two months) and smaller particle sizes, which enhance skin penetration and sustain drug release.95 However, these formulations exhibit increased leakage and degradation at elevated storage temperatures. This temperature-dependent instability is attributed to increased lipid fluidity which facilitates drug leakage, underscoring the importance of maintaining storage conditions at 4 °C to ensure product stability.
In a 12 weeks split-face clinical study involving 30 women, Banihashemi et al96 evaluated 5% topical liposomal TA with no reported discomfort while yielding significant superior MASI scores reduction as compared to conventional treatments. These findings highlight its potential as a novel and safe therapeutic modality for melasma. Similarly, a study using 1.8% liposomal TA in 60 patients with melasma demonstrated over 50% improvement, further supporting its efficacy.97 Furthermore, Politranexamide® which is a patented liposomal TA emulsion achieved a significant MASI score reduction from 10.73 to 7.75 in facial melasma treatment.98 Choo and Tey93 conducted a comprehensive study evaluating the in vitro skin-lightening effects of TA encapsulated in poly(lactic-co-glycolic acid) (PLGA)-based polymeric nanoparticles and in liposomes. Liposomal-TA demonstrated superior efficacy, achieving greater reduction in melanin content despite containing only half the concentration of TA (0.25% vs 0.5%) as compared with PLGA-TA. This enhanced penetration may be attributed to the compositional similarity between liposomal phospholipids to skin membrane lipids, which facilitates permeation across the SC via both intracellular and transcellular pathways.92
Ethosomes
Ethosomes are specialized lipidic vesicles containing phospholipids, water and 20-45% (v/v) ethanol, first reported by Touitou et al75 which markedly improve transdermal drug delivery.76 According to studies, the interaction between ethanol, vesicles and skin’s lipid bilayer significantly impact SC fluidity, enhances skin compatibility and drug penetration. Its mechanism of action involves ethanol-induced SC lipid fluidisation, dissolution of intercellular lipids and a downward shift in the SC-phase transition temperature thereby increasing membrane permeability, facilitating drug penetration and retention.99-102 Compared with liposomes (EE ≈ 60-70%), ethosomes exhibit 1.5-2 times higher entrapment efficiency (EE ≈ 85-95%) and 3-4 times greater deformability index, enabling 2-6 times deeper permeation into viable epidermis in ex-vivo Franz-cell studies utilising excised rat skin.103 They outperform conventional liposomes in exhibiting higher drug-entrapment efficiency and superior deformability, facilitating the efficient delivery of water and lipid soluble drugs through the SC into deeper viable layers of the skin.75,104,105 Consequently, ethosomes have been investigated for various skin conditions treatment including acne, psoriasis, melasma and atopic dermatitis, yet < 10% of these studies have progressed beyond ex-vivo human to controlled clinical trials.106
Nonetheless, the presence of ethanol in ethosomes formulation possess several drawbacks including volatility, risk of cutaneous irritation and reduced stability which may negatively impact formulation quality and shelf life. In contrast, Mehmood et al107 reported that a vitamin D-loaded ethosomal gel did not produce any irritation on rabbit skin after 24 hours of application in their in vivo study. These findings suggest that ethosomes may be considered relatively safe and non-toxic for topical use. An increase in ethanol concentration has been shown to improve drug molecules diffusion across skin barrier with optimal effects observed at concentrations up to 30%. This enhancement is attributed to ethanol’s ability to fluidize lipid bilayers and increase membrane permeability. However, further increase of ethanol content beyond 30% specifically at 45% has been reported to inhibit the diffusion efficiency of the active compound due to excessive permeability of the ethosomal membrane.77 This destabilization of the ethosomes structure ultimately compromises the integrity and performance of the delivery system.102 Hence, modified ethosomal systems utilizing propylene-glycol, glycerol or phytoconstituent such as curcumin have been developed as ethanol substitutes with the purpose of mitigating these limitations. These alternatives provide better stability, lower volatility and enhanced sensitive skin compatibility.108,109
A study by Niu et al110 demonstrated that drug-loaded ethosomes fusing with SC lipids and breaching the barrier to reach the viable epidermis with an EE of 78.21% and up to 95% of drug permeation in ex-vivo transdermal diffusion cell study in excised pig skin. Furthermore, Guo et al29 conducted a randomized double-blind clinical trial (n = 88, Fitzpatrick III-IV) investigating 0.5% TA-loaded ethosomes with 30% ethanol for melasma. Results showed that vascularization-related melasma significantly improved in the TA-loaded ethosomes group likely due to the elevated ethanol concentration which disrupts the SC enhancing drug delivery by passive transport.111 Shaji and Parab112 introduced transethosomes (ethosomes containing edge activators) that achieved 94% of EE and 93.97% in TA deposition within the viable epidermis in excised porcine abdomen skin showing enhanced flexibility and penetration capability. These optimized ethosomes offer a simple production process, improved scalability and a reduced TA dosage requirement, thereby minimizing toxicity risks and improving patient compliance.113 However, TA-loaded ethosomes have received limited research attention compared to other drugsand further clinical studies with objective biomarkers and irritation scoring are necessary to thoroughly evaluate their safety and effectiveness against melasma.114-116
Niosomes
Niosomes are described as nanocarrier vesicles that are formed through the self-assembly of non-ionic surfactants with size distributions between 10 and 1000 nm. The surfactants most utilised in niosomes are polyoxyethylene alkyl ethers and sorbitan esters which are non-toxic, biodegradable, biocompatible and chemically stable.78,79 For instance, span60/cholesterol-based niosomes loaded with mangosteen extract for wound healing applications preserved ≥ 80% viability of murine fibroblast cells across all tested concentrations (10%-100%) and were classified as non-irritating in in vivo rabbit skin studies. The reported irritation index was 0.29, with no observable signs of erythema or oedema up to 72 hours post-application.117 Research on niosomes has substantially increased in recent years due to their nanoscale size and amphiphilic characteristics which permit the encapsulation of a wide range of pharmacological molecules and enhances cutaneous penetration.118 Niosomes were designed as chemically stable and economical liposomes substitutes, offering improved bilayer rigidity and achieving up to 90% entrapment efficiency with approximately 85% drug release.119 Unlike liposomes, niosomes avoid oxidative degradation, reduce raw material costs by 30%-50% and minimize variability by replacing oxidation-prone phospholipids with non-ionic surfactants.66,80 Furthermore, niosomes functions as intradermal drug depots, facilitating sustained drug release and enable targeted delivery while reducing dosage requirements.120-123 Its mechanism of action involves surfactants-induced SC lipid fusion and modification of thermodynamic activity gradient thereby promoting transdermal drug penetration.68,124,125
Niosomes were first identified for cosmetic applications in 1972. However, peer-reviewed investigations specifically addressing TA-loaded niosomes remain limited with ≤ 10 studies indexed in PubMed/Web of Science as of July 2024, highlighting a critical knowledge gap that requires systematic exploration. The first commercial niosomal anti-aging cream was introduced by Lancôme in 1987, followed by L’Oréal’s patented “NiosômeTM” technology which further validated industrial-scale reproducibility with > 95 % batch uniformity.126,127 Given their unique physicochemical properties, niosomes have been widely studied as delivery systems for active compounds including cannabidiol, forskolin, caffeine and aescin, offering hydrating, anti-aging, antioxidant, anti-inflammatory and skin-whitening benefits.124,128,129 Their ability to improve chemical stability and enhance cutaneous absorption especially for poorly soluble drugs, makes them highly attractive for cosmetic and dermatological applications.130,131 In a study published in 2010, Shatalebi et al132 demonstrated that N-acetyl glucosamine-loaded niosomes (500-4500 nm) increased skin retention by 42% relative to control solution and maintained up to 24 hours of steady-state flux, indicating promising efficacy for hyperpigmentation treatment.
Further studies have investigated the development of hydroquinone-loaded niosomal gel to enhance skin depigmentation. Hydroquinone is a commonly used depigmenting agent where excessive concentrations may cause skin irritation including burning and redness. Ammar et al133 formulated a Span-80/cholesterolniosomal topical gel with 98% of EE and achieving97% in vitro hydroquinone release. A randomized comparative clinical trial further demonstrated up to 85% improvement in therapeutic impact over 12 weeks treatment period. This trial also reported minimal to no adverse effects, which were attributed to the high encapsulation efficiency in niosomes that reduce hydroquinone direct contact on skin. Similar findings were also reported by Divanbeygikermani et al.134 Moreover, several other studies have also confirmed the efficacy of niosomes in cosmeceutical applications.135,136 Focusing on transdermal delivery, niosomes has outperformed both liposomes and ethosomes in terms of drug release kinetics and entrapment efficacy. This is primarily attributed to surfactants incorporation which stabilizes vesicle membrane and impart high deformability, hence enhancing penetration through SC bypass.137 Nevertheless, optimization of niosomes’ formulation specifically TA-loaded remain under-investigated.138 Systematic investigations are required to determine the optimal surfactant-to-cholesterol molar ratios, preparation methods and concentration of TA to facilitate clinical translation for hyperpigmentation and melasma treatment.
Transferosomes
Transferosomes are recognized as a novel variant of liposomes distinguished by their superior deformability. They are primarily composed of phospholipids forming a bilayer membrane, an edge activator (10%-25%), ethanol ( < 10%), and water as the dispersion medium. These vesicles typically exhibit particle sizes under 300 nm, possess exceptional elasticity through the incorporation of edge activators that destabilize and alter the lipid bilayer. Commonly employed edge activators comprise non-ionic surfactants (Tweens, Spans) and bile salts (etc. sodium deoxycholate).66 Structurally, transferosomes consist of a phospholipid bilayer enclosed aqueous core where hydrophilic active agents are encapsulated in the core and hydrophobic compounds are solubilized within the membrane. The inclusion of edge activators reduces interfacial tension and alters bilayer assembly, making transferosomes highly malleable and capable of intercalating into the SC lipid matrix without compromising vesicle integrity or cargo retention.67 This extreme deformability enables transferosomes to bypass the SC barrier, where they gradually release their payload into deeper skin layers while simultaneously protecting the active compounds from metabolic degradation.81
In comparison to conventional liposomes, transferosomes are not only non-toxic, biocompatible and biodegradable but also exhibit superior physical stability and enhanced transdermal penetration efficiency.82 In a study by Wadher et al,139 blank phospholipid/sodium-deoxycholate transferosomes exhibited no cytotoxic effects on normal human cell lines across concentrations ranging from 0-15 mg/mL. Given their superior deformability and non-cytotoxicity, transferosomes are particularly suitable for cosmeceutical applications, especially in the topical delivery of antioxidants. For instance, Li et al140 developed ascorbic palmitate (AP)-loaded for improved melasma treatment. Both in-vitro and in-vivo studies demonstrated a 14.1-fold increase in AP skin permeability and superior anti-melasma efficacy, with effective attenuation of oxidative stress and inflammation, and no observable signs of skin irritation. Similarly, Lee et al141 formulated niacinamide-loaded transferosomes which demonstrated markedly enhanced skin penetration and whitening efficacy relative to conventional liposomes, highlighting their potential in melasma and hyperpigmentation management. However, to date, the development of TA-loaded transferosomes remains largely unexplored. Owing to the high deformability of transferosomes, it is scientifically reasonable that TA-loaded transferosomes could bypass the SC and enhanced transdermal absorption efficacy,82 where further investigation is required.
Phytosomes
Phytosomes also known as phytophospholipid complexes, are advanced lipidic vesicular systems that integrate phospholipids with biologically active phytochemicals through bonding of hydrogen, typically between the hydrophilic regions of both molecules. This delivery technology was first introduced by Indena Company in the late 1980s to address poor oral bioavailability of certain plant-derived compounds that suffer from extensive first-pass metabolism and limited membrane permeability which restricts their therapeutic potential.83 Structurally, phytosomes resemble conventional liposomes but offering more advantages, including higher encapsulation efficiency, superior physicochemical stability and significantly enhanced absorption and bioavailability of active ingredients.84 Transdermal delivery of bioactive molecules via phytosomes can occur through various pathways across the SC including intercellular (sweat and sebaceous glands, hair follicles) and intracellular (lipid matrix and corneocytes) routes. It has been reported that drug encapsulation within phytosomes results in a lipid-soluble complex that can interact with both lipid and water-based environments thereby increasing the drug’s diffusion coefficient and enhancing its partitioning into the SC can significantly improve skin permeability.142,143
Phytosomes are typically fabricated within a particle size range of 50 nm to several 100mm, allowing for formulation flexibility tailored to specific application requirements.83 Over the past decade, numerous botanical extracted phytochemicals have been successfully incorporated into phytosomes for both dermatological and cosmetic applications. For instance, Priani et al144 formulated a topical phytosome serum loaded with cocoa-pod extract which demonstrated high EE of 91% with a particle size of 672 nm. This formulation also exhibited strong antioxidant activity with an IC50 value of 199.98 ppm which is comparable to a commercial whitening product (Hadalabo Ultimate Whitening Milk). Similarly, Patel et al145 developed and optimized arbutin/phosphatidylcholine complexes to address the limited skin permeability of arbutin as a skin-whitening agent. The optimized formulation showed an enhanced in-vitro drug release profile as compared to aqueous formulation (84.8% vs 53.15%), indicating improved cutaneous absorption. In comparison to other vesicular carriers, phytosomes represent a unique class of bioactive delivery systems in which the phospholipids not only serve as a vehicle but also exhibit membrane-repair and anti-inflammatory benefits.146 Therefore, the integration of phytosomes with TA may present promising approach to improve skin permeability and bioavailability while potentially exerting synergistic effects through both active components.
Limitations and Challenges
Lipid-based vesicular drug delivery systems have attracted considerable attention in contemporary research, particularly in dermatology and cosmeceuticals. Nonetheless, the development of TA-loaded lipidic vesicles faces substantial challenges in formulation, regulation and clinical translation. From a formulation perspective, liposomal TA requires ≥ 98% of ultra-pure phospholipids and specialized techniques such as thin-film hydration, both of which significantly increase production costs.147 In addition, liposomes are highly susceptible to oxidation and degradation which compromises long-term stability. Ethosomes containing > 30% ethanol also exhibit reduced stability and drug leakage under elevated temperature or humidity, complicating storage and transportation. High ethanol concentrations may further induce skin irritation or erythema if not carefully optimized and can negatively impact drug solubility, stability and bioavailability.148 Other vesicular systems including transferosomes, niosomes and phytosomes present additional challenges related to complex physicochemical behaviour, excipient interactions and a lack of robust in vivo safety data. In particular, the edge activators and surfactants utilised which are essential for improving deformability and penetration may also pose long-term toxicity risks if not optimized.149
Beyond formulation, regulatory gaps further complicate translation. Currently, no country has established legislation specifically dedicated to nano-systems in dermatology or cosmetics. For instance, neither the U.S. Food and Drug Administration (FDA) nor the Malaysian National Pharmaceutical Regulatory Agency (NPRA) has developed comprehensive guidelines for functional cosmetics employing vesicular nanocarriers. Lipidic vesicular formulations are classified as non-biological complex drugs (NBCDs) requiring robust characterisation of primary quality indicators such as particle size, zeta potential, encapsulation efficiency and lipid composition.150,151 Additionally, FDA has published a guidance specifically for generic liposomes to enhance research quality, consumer transparency and regulatory rigor.152 However, no equivalent framework exists for other lipid-based nano-systems which continue to be investigated and marketed with comparatively fewer regulatory safeguards.130
Furthermore, although formulation and regulatory barriers are being addressed, the clinical evidence for TA-loaded vesicular systems remains insufficient. Most trials are underpowered, with nearly 90% enrolling fewer than 100 participants. The largest study of n = 88 reported MASI score reduction by 48%, but with wide confidence interval (21%-75%) and low statistical power (β = 0.26) limit reliability.86 Besides that, follow-up intervals are relatively short ≤ 12 weeks) preventing evaluation of long-term risks such as rebound pigmentation, ethanol-induced SC barrier disruption and rare thromboembolic events.18,29,99 Methodological inconsistencies also further undermine validity where outcome measures vary between modified MASI and global 5-point physician scales, while standardised photography and objective tools such as dermoscopy or Wood’s lamp necessary for differentiating between epidermal and dermal forms of melasma are rarely incorporated.29,105 Therefore, addressing these gaps will be critical for TA-loaded vesicular systems to progress from experimental formulations to guideline-supported therapies for melasma.
Conclusion
Melasma is a chronic and relapsing skin disorder that is multifactorial in origin involving prolonged UVR exposure, genetic susceptibility, hormonal fluctuations and hyperpigmentation triggered by medications or underlying illnesses. Despite advancements in technology and drug development, effective treatment remains challenging. A wide range of interventions including topical formulations, systemic medications and procedural interventions have been explored but many of them demonstrate limited clinical efficacy, high rate of recurrence and undesirable side effects. TA has recently gained recognition as a promising melasma therapeutic option with extensive research conducted on different TA formulations, particularly oral and topical applications. While topical TA alone is considered less effective, it is often preferred due to better patient compliance and lesser side effects. Lipidic vesicular system incorporated with TA represents a promising advancement in melasma treatment, offering enhanced delivery profile, minimized adverse effects and enhanced patient compliance in comparison to conventional methods. However, clinical application remains hindered by several critical challenges: (i) the high cost manufacturing and regulatory complexity, (ii) limited shelf-life and temperature-dependent formulation stability, and (iii) the absence of standardized, validated quality control assays for vesicle characterisation and drug release.
Future Perspectives
Moving forward, TA’s incorporation within lipidic vesicles alongside complementary therapeutics such as hyaluronic acid (HA) and microneedle holds potential for optimizing treatment outcomes. These approaches may enhance drug absorption, improve skin hydration and promote overall skin health. Furthermore, innovations in lipidic vesicular nanotechnology could pave the way for personalized dermatological treatments. Future TA formulations may be customized to different types of skin, melasma severity and genetic predispositions, potentially enhancing therapeutic outcomes and patient satisfaction. While significant progress has been made, further research especially multicentred, randomized and dose-ranging clinical trials are needed to optimize standardized protocols, incorporate long-term safety monitoring as well as explore new therapeutic possibilities. Nevertheless, this article underscores the potential of lipidic vesicular formulations for TA to emerge as the first line melasma treatment in the foreseeable future (Supplementary file 1, Table S1). This advancement is contingent upon continued innovation and collaborative efforts within the field to hold the promise of delivering safer, more effective and personalized treatment options to patients.
Competing Interests
The authors have no conflicts of interest to declare.
Ethical Approval
Not applicable.
Supplementary Files
Supplementary file 1 contains Table S1.
(pdf)
References
- Zhu JW, Ni YJ, Tong XY, Guo X, Wu XP, Lu ZF. Tranexamic acid inhibits angiogenesis and melanogenesis in vitro by targeting VEGF receptors. Int J Med Sci 2020; 17(7):903-11. doi: 10.7150/ijms.44188 [Crossref] [ Google Scholar]
- Jusuf NK, Putra IB, Mahdalena M. Is there a correlation between severity of melasma and quality of life?. Open Access Maced J Med Sci 2019; 7(16):2615-8. doi: 10.3889/oamjms.2019.407 [Crossref] [ Google Scholar]
- Basit H, Godse KV, Al Aboud AM. Melasma. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459271/.
- Grimes PE, Ijaz S, Nashawati R, Kwak D. New oral and topical approaches for the treatment of melasma. Int J Womens Dermatol 2019; 5(1):30-6. doi: 10.1016/j.ijwd.2018.09.004 [Crossref] [ Google Scholar]
- Passeron T, Picardo M. Melasma, a photoaging disorder. Pigment Cell Melanoma Res 2018; 31(4):461-5. doi: 10.1111/pcmr.12684 [Crossref] [ Google Scholar]
- Thawabteh AM, Jibreen A, Karaman D, Thawabteh A, Karaman R. Skin pigmentation types, causes and treatment-a review. Molecules 2023; 28(12):4839. doi: 10.3390/molecules28124839 [Crossref] [ Google Scholar]
- Arellano I, Cestari T, Ocampo-Candiani J, Azulay-Abulafia L, Bezerra Trindade Neto P, Hexsel D. Preventing melasma recurrence: prescribing a maintenance regimen with an effective triple combination cream based on long-standing clinical severity. J Eur Acad Dermatol Venereol 2012; 26(5):611-8. doi: 10.1111/j.1468-3083.2011.04135.x [Crossref] [ Google Scholar]
- Han HJ, Kim JC, Park YJ, Kang HY. Targeting the dermis for melasma maintenance treatment. Sci Rep 2024; 14(1):949. doi: 10.1038/s41598-023-51133-w [Crossref] [ Google Scholar]
- Andrus E. New Trio Combination Cream Efficacious in Melasma Treatment. Dermatology Times; 2023. Available from: https://www.dermatologytimes.com/view/new-trio-combination-cream-efficacious-in-melasma-treatment. Accessed June 17, 2024.
- Bertold C, Fontas E, Singh T, Gastaut N, Ruitort S, Wehrlen Pugliese S. Efficacy and safety of a novel triple combination cream compared to Kligman’s trio for melasma: a 24-week double-blind prospective randomized controlled trial. J Eur Acad Dermatol Venereol 2023; 37(12):2601-7. doi: 10.1111/jdv.19455 [Crossref] [ Google Scholar]
- Piquero-Casals J, Granger C, Piquero-Casals V, Garre A, Mir-Bonafé JF. A treatment combination of peels, oral antioxidants, and topical therapy for refractory melasma: a report of 4 cases. Clin Cosmet Investig Dermatol 2020; 13:209-13. doi: 10.2147/ccid.S242180 [Crossref] [ Google Scholar]
- Gharib K, Morsi HM. Treatment of melasma with intralesional tranexamic acid versus cryotherapy. J Clin Aesthet Dermatol 2022; 15(2):44-8. [ Google Scholar]
- Chauncey JM, Patel P. Tranexamic acid. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532909/.
- Wang WJ, Wu TY, Tu YK, Kuo KL, Tsai CY, Chie WC. The optimal dose of oral tranexamic acid in melasma: a network meta-analysis. Indian J Dermatol Venereol Leprol 2023; 89(2):189-94. doi: 10.25259/ijdvl_530_2021 [Crossref] [ Google Scholar]
- Kim KM, Lim HW. The uses of tranexamic acid in dermatology: a review. Int J Dermatol 2023; 62(5):589-98. doi: 10.1111/ijd.16160 [Crossref] [ Google Scholar]
- Maeda K. Mechanism of action of topical tranexamic acid in the treatment of melasma and sun-induced skin hyperpigmentation. Cosmetics 2022; 9(5):108. doi: 10.3390/cosmetics9050108 [Crossref] [ Google Scholar]
- Lee HC, Thng TG, Goh CL. Oral tranexamic acid (TA) in the treatment of melasma: a retrospective analysis. J Am Acad Dermatol 2016; 75(2):385-92. doi: 10.1016/j.jaad.2016.03.001 [Crossref] [ Google Scholar]
- Del Rosario E, Florez-Pollack S, Zapata L Jr, Hernandez K, Tovar-Garza A, Rodrigues M. Randomized, placebo-controlled, double-blind study of oral tranexamic acid in the treatment of moderate-to-severe melasma. J Am Acad Dermatol 2018; 78(2):363-9. doi: 10.1016/j.jaad.2017.09.053 [Crossref] [ Google Scholar]
- Wu S, Shi H, Wu H, Yan S, Guo J, Sun Y. Treatment of melasma with oral administration of tranexamic acid. Aesthetic Plast Surg 2012; 36(4):964-70. doi: 10.1007/s00266-012-9899-9 [Crossref] [ Google Scholar]
- Na JI, Choi SY, Yang SH, Choi HR, Kang HY, Park KC. Effect of tranexamic acid on melasma: a clinical trial with histological evaluation. J Eur Acad Dermatol Venereol 2013; 27(8):1035-9. doi: 10.1111/j.1468-3083.2012.04464.x [Crossref] [ Google Scholar]
- Agrawal M, Varma K, Kumar U, Bhargava S, Mahadik A, Agrawal V. Comparison of oral versus topical tranexamic acid for treatment of melasma. IP Indian J Clin Exp Dermatol 2023; 9(2):84-89. doi: 10.18231/j.ijced.2023.015 [Crossref] [ Google Scholar]
- Khan AS, Sathyanath A, Kurian AM, Mohanty P, Bisoyi D, Mohanty J. Comparing oral tranexamic acid and Q-switched Nd-YAG laser for melasma: a randomized study. SSR Inst Int J Life Sci 2024; 10(1):3590-8. doi: 10.21276/ssr-iijls.2024.10.1.21 [Crossref] [ Google Scholar]
- Higashi N. Treatment of melasma with oral tranexamic acid. Skin Res 1988; 30(5):676-80. doi: 10.11340/skinresearch1959.30.676 [Crossref] [ Google Scholar]
- Kim SJ, Park JY, Shibata T, Fujiwara R, Kang HY. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin Exp Dermatol 2016; 41(5):480-5. doi: 10.1111/ced.12835 [Crossref] [ Google Scholar]
- Fox C. From Tranexamic Acid on Freckles to Nonanimal Fillers: Patent, Literature Findings. Cosmetics & Toiletries; 2008. Available from: https://www.cosmeticsandtoiletries.com/research/literature-data/article/21834182/from-tranexamic-acid-on-freckles-to-nonanimal-fillers-patent-literature-findings. Accessed June 18, 2024.
- Atefi N, Dalvand B, Ghassemi M, Mehran G, Heydarian A. Therapeutic effects of topical tranexamic acid in comparison with hydroquinone in treatment of women with melasma. Dermatol Ther (Heidelb) 2017; 7(3):417-24. doi: 10.1007/s13555-017-0195-0 [Crossref] [ Google Scholar]
- Yoo J, Ahn H, Kim MS, Jue MS, Choi KH. Efficacy of topical tranexamic acid in treatment of melasma. Korean J Dermatol 2017; 55(5):283-9. [ Google Scholar]
- Ogbechie-Godec OA, Elbuluk N. Melasma: an up-to-date comprehensive review. Dermatol Ther (Heidelb) 2017; 7(3):305-18. doi: 10.1007/s13555-017-0194-1 [Crossref] [ Google Scholar]
- Guo Q, Hu D, Pei Q, Wang S, Yan M, Dong J. Effects of masks containing 05% tranexamic acid-loaded ethosomes on melasma in the Asian skin: a randomized controlled clinical trial. Dermatol Ther (Heidelb) 2023; 2023(1):1917453. doi: 10.1155/2023/1917453 [Crossref] [ Google Scholar]
- Kadhum WR, Sekiguchi S, Hijikuro I, Todo H, Sugibayashi K. A novel chemical enhancer approach for transdermal drug delivery with C17-monoglycerol ester liquid crystal-forming lipid. J Oleo Sci 2017; 66(5):443-54. doi: 10.5650/jos.ess16204 [Crossref] [ Google Scholar]
- Liu Y, Han Y, Zhu T, Wu X, Yu W, Zhu J. Targeting delivery and minimizing epidermal diffusion of tranexamic acid by hyaluronic acid-coated liposome nanogels for topical hyperpigmentation treatment. Drug Deliv 2021; 28(1):2100-7. doi: 10.1080/10717544.2021.1983081 [Crossref] [ Google Scholar]
- Nassar A, Gharib K, Abdel-Azim B, Akl M. Tranexamic acid, a promising melasma treatment modality; past and future treatment regimen. Zagazig Univ Med J 2024;30(1.2):80-7. doi: 10.21608/zumj.2022.120349.2471.
- Panchal VS, Patel YS, Dalal YD, Parikh AP, Dalal AD, Rana DA. Efficacy of oral, topical, and intradermal tranexamic acid in patients with melasma - a meta-analysis. Indian Dermatol Online J 2024; 15(1):55-63. doi: 10.4103/idoj.idoj_495_22 [Crossref] [ Google Scholar]
- Espósito AC, Cassiano DP, da Silva CN, Lima PB, Dias JA, Hassun K. Update on melasma—part I: pathogenesis. Dermatol Ther (Heidelb) 2022; 12(9):1967-88. doi: 10.1007/s13555-022-00779-x [Crossref] [ Google Scholar]
- Alcantara GP, Esposito AC, Olivatti TO, Yoshida MM, Miot HA. Evaluation of ex vivo melanogenic response to UVB, UVA, and visible light in facial melasma and unaffected adjacent skin. An Bras Dermatol 2020; 95(6):684-90. doi: 10.1016/j.abd.2020.02.015 [Crossref] [ Google Scholar]
- Sarkar R, Puri P, Jain RK, Singh A, Desai A. Melasma in men: a clinical, aetiological and histological study. J Eur Acad Dermatol Venereol 2010; 24(7):768-72. doi: 10.1111/j.1468-3083.2009.03524.x [Crossref] [ Google Scholar]
- Mahajan VK, Patil A, Blicharz L, Kassir M, Konnikov N, Gold MH. Medical therapies for melasma. J Cosmet Dermatol 2022; 21(9):3707-28. doi: 10.1111/jocd.15242 [Crossref] [ Google Scholar]
- Bajpai VK, Swigut T, Mohammed J, Naqvi S, Arreola M, Tycko J. A genome-wide genetic screen uncovers determinants of human pigmentation. Science 2023; 381(6658):eade6289. doi: 10.1126/science.ade6289 [Crossref] [ Google Scholar]
- Lee AY. Recent progress in melasma pathogenesis. Pigment Cell Melanoma Res 2015; 28(6):648-60. doi: 10.1111/pcmr.12404 [Crossref] [ Google Scholar]
- Ortonne JP, Arellano I, Berneburg M, Cestari T, Chan H, Grimes P. A global survey of the role of ultraviolet radiation and hormonal influences in the development of melasma. J Eur Acad Dermatol Venereol 2009; 23(11):1254-62. doi: 10.1111/j.1468-3083.2009.03295.x [Crossref] [ Google Scholar]
- de Almeida Tamega A, Miot LD, Bonfietti C, Gige TC, Marques ME, Miot HA. Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women. J Eur Acad Dermatol Venereol 2013; 27(2):151-6. doi: 10.1111/j.1468-3083.2011.04430.x [Crossref] [ Google Scholar]
- Naik PP, Farrukh SN. Influence of ethnicities and skin color variations in different populations: a review. Skin Pharmacol Physiol 2022; 35(2):65-76. doi: 10.1159/000518826 [Crossref] [ Google Scholar]
- Brenner M, Hearing VJ. The protective role of melanin against UV damage in human skin. Photochem Photobiol 2008; 84(3):539-49. doi: 10.1111/j.1751-1097.2007.00226.x [Crossref] [ Google Scholar]
- McLeod SD, Ranson M, Mason RS. Effects of estrogens on human melanocytes in vitro. J Steroid Biochem Mol Biol 1994; 49(1):9-14. doi: 10.1016/0960-0760(94)90295-x [Crossref] [ Google Scholar]
- Azzahra CN, Widyawati W, Afriliana L, Dewantiningrum J. Melasma show up in contraceptive pills acceptors. Jurnal Kedokteran Diponegoro (Diponegoro Medical Journal) 2021; 10(1):74-7. doi: 10.14710/dmj.v10i1.29436 [Crossref] [ Google Scholar]
- Jang YH, Lee JY, Kang HY, Lee ES, Kim YC. Oestrogen and progesterone receptor expression in melasma: an immunohistochemical analysis. J Eur Acad Dermatol Venereol 2010; 24(11):1312-6. doi: 10.1111/j.1468-3083.2010.03638.x [Crossref] [ Google Scholar]
- Lieberman R, Moy L. Estrogen receptor expression in melasma: results from facial skin of affected patients. J Drugs Dermatol 2008; 7(5):463-5. [ Google Scholar]
- Liu W, Chen Q, Xia Y. New mechanistic insights of melasma. Clin Cosmet Investig Dermatol 2023; 16:429-42. doi: 10.2147/ccid.S396272 [Crossref] [ Google Scholar]
- Maddaleno AS, Camargo J, Mitjans M, Vinardell MP. Melanogenesis and melasma treatment. Cosmetics 2021; 8(3):82. doi: 10.3390/cosmetics8030082 [Crossref] [ Google Scholar]
- Kim NH, Cheong KA, Lee TR, Lee AY. PDZK1 upregulation in estrogen-related hyperpigmentation in melasma. J Invest Dermatol 2012; 132(11):2622-31. doi: 10.1038/jid.2012.175 [Crossref] [ Google Scholar]
- Cario M. How hormones may modulate human skin pigmentation in melasma: an in vitro perspective. Exp Dermatol 2019; 28(6):709-18. doi: 10.1111/exd.13915 [Crossref] [ Google Scholar]
- Bala HR, Lee S, Wong C, Pandya AG, Rodrigues M. Oral tranexamic acid for the treatment of melasma: a review. Dermatol Surg 2018; 44(6):814-25. doi: 10.1097/dss.0000000000001518 [Crossref] [ Google Scholar]
- Loner C, Estephan M, Davis H, Cushman JT, Acquisto NM. Effect of fluctuating extreme temperatures on tranexamic acid. Prehosp Disaster Med 2019; 34(3):340-2. doi: 10.1017/s1049023x19004308 [Crossref] [ Google Scholar]
- Sarkar R, Chugh S, Garg VK. Newer and upcoming therapies for melasma. Indian J Dermatol Venereol Leprol 2012; 78(4):417-28. doi: 10.4103/0378-6323.98071 [Crossref] [ Google Scholar]
- Khuraiya S, Kachhawa D, Chouhan B, Dua M, Rao P. A comparative study of topical 5% tranexamic acid and triple combination therapy for the treatment of melasma in Indian population. Pigment Int 2019.6(1):18-23. doi: 10.4103/Pigmentinternational.Pigmentinternational_26_17.
- Babbush KM, Babbush RA, Khachemoune A. The therapeutic use of antioxidants for melasma. J Drugs Dermatol 2020; 19(8):788-92. doi: 10.36849/jdd.2020.5079 [Crossref] [ Google Scholar]
- Cho YH, Park JE, Lim DS, Lee JS. Tranexamic acid inhibits melanogenesis by activating the autophagy system in cultured melanoma cells. J Dermatol Sci 2017; 88(1):96-102. doi: 10.1016/j.jdermsci.2017.05.019 [Crossref] [ Google Scholar]
- Maeda K, Tomita Y. Mechanism of the inhibitory effect of tranexamic acid on melanogenesis in cultured human melanocytes in the presence of keratinocyte-conditioned medium. J Health Sci 2007; 53(4):389-96. doi: 10.1248/jhs.53.389 [Crossref] [ Google Scholar]
- Maeda K, Naganuma M. Topical trans-4-aminomethylcyclohexanecarboxylic acid prevents ultraviolet radiation-induced pigmentation. J Photochem Photobiol B 1998; 47(2-3):136-41. doi: 10.1016/s1011-1344(98)00212-7 [Crossref] [ Google Scholar]
- Karthikeyan M, Kumar GJ, Radhakrishnan I. A comparison of the effectiveness of intralesional tranexamic acid against platelet-rich plasma in the treatment of melasma. Int J Res Dermatol 2024; 10(3):126-31. doi: 10.18203/issn.2455-4529.IntJResDermatol20240970 [Crossref] [ Google Scholar]
- Renckens R, Weijer S, de Vos AF, Pater JM, Meijers JC, Hack CE. Inhibition of plasmin activity by tranexamic acid does not influence inflammatory pathways during human endotoxemia. Arterioscler Thromb Vasc Biol 2004; 24(3):483-8. doi: 10.1161/01.Atv.0000118280.95422.48 [Crossref] [ Google Scholar]
- Poojary S, Minni K. Tranexamic acid in melasma: a review. Pigment Disord 2015; 2(12):228. doi: 10.4172/2376-0427.1000228 [Crossref] [ Google Scholar]
- González-Molina V, Martí-Pineda A, González N. Topical treatments for melasma and their mechanism of action. J Clin Aesthet Dermatol 2022; 15(5):19-28. [ Google Scholar]
- Bhattacharjee R, Hanumanthu V, Thakur V, Bishnoi A, Vinay K, Kumar A. A randomized, open-label study to compare two different dosing regimens of oral tranexamic acid in treatment of moderate to severe facial melasma. Arch Dermatol Res 2023; 315(6):1831-6. doi: 10.1007/s00403-023-02549-x [Crossref] [ Google Scholar]
- Zhu CY, Li Y, Sun QN, Takada A, Kawada A. Analysis of the effect of different doses of oral tranexamic acid on melasma: a multicentre prospective study. Eur J Dermatol 2019; 29(1):55-8. doi: 10.1684/ejd.2018.3494 [Crossref] [ Google Scholar]
- Jain S, Jain V, Mahajan SC. Lipid based vesicular drug delivery systems. Advances in Pharmaceutics 2014; 2014(1):574673. doi: 10.1155/2014/574673 [Crossref] [ Google Scholar]
- Garg U, Jain K. Dermal and transdermal drug delivery through vesicles and particles: preparation and applications. Adv Pharm Bull 2022; 12(1):45-57. doi: 10.34172/apb.2022.006 [Crossref] [ Google Scholar]
- Gaur PK, Minocha S, Mishra R, Lal N, Lata K. Recent Advances in development of vesicular carrier for transdermal drug delivery: a review. Jordan J Pharm Sci 2024; 17(1):1-30. doi: 10.35516/jjps.v17i1.1313 [Crossref] [ Google Scholar]
- Kumar B, Pandey M, Aggarwal R, Sahoo PK. A comprehensive review on invasomal carriers incorporating natural terpenes for augmented transdermal delivery. Futur J Pharm Sci 2022; 8(1):50. doi: 10.1186/s43094-022-00440-6 [Crossref] [ Google Scholar]
- Zou L, Cheng M, Hu K, Feng J, Tu L. Vesicular drug delivery systems for oral absorption enhancement. Chin Chem Lett 2024; 35(7):109129. doi: 10.1016/j.cclet.2023.109129 [Crossref] [ Google Scholar]
- Budai M, Szógyi M. [Liposomes as drug carrier systems. Preparation, classification and therapeutic advantages of liposomes]. Acta Pharm Hung 2001;71(1):114-8. [Hungarian].
- Bozzuto G, Molinari A. Liposomes as nanomedical devices. Int J Nanomedicine 2015; 10:975-99. doi: 10.2147/ijn.S68861 [Crossref] [ Google Scholar]
- Basak S, Das TK. Liposome-based drug delivery systems: from laboratory research to industrial production—instruments and challenges. ChemEngineering 2025; 9(3):56. doi: 10.3390/chemengineering9030056 [Crossref] [ Google Scholar]
- Sharma VK, Agrawal MK. A historical perspective of liposomes-a bio nanomaterial. Mater Today Proc 2021; 45(Pt 2):2963-6. doi: 10.1016/j.matpr.2020.11.952 [Crossref] [ Google Scholar]
- Touitou E, Dayan N, Bergelson L, Godin B, Eliaz M. Ethosomes - novel vesicular carriers for enhanced delivery: characterization and skin penetration properties. J Control Release 2000; 65(3):403-18. doi: 10.1016/s0168-3659(99)00222-9 [Crossref] [ Google Scholar]
- Bendas ER, Tadros MI. Enhanced transdermal delivery of salbutamol sulfate via ethosomes. AAPS PharmSciTech 2007; 8(4):E107. doi: 10.1208/pt0804107 [Crossref] [ Google Scholar]
- Pilch E, Musiał W. Liposomes with an ethanol fraction as an application for drug delivery. Int J Mol Sci 2018; 19(12):3806. doi: 10.3390/ijms19123806 [Crossref] [ Google Scholar]
- Ag Seleci D, Seleci M, Walter JG, Stahl F, Scheper T. Niosomes as nanoparticular drug carriers: fundamentals and recent applications. J Nanomater 2016; 2016(1):7372306. doi: 10.1155/2016/7372306 [Crossref] [ Google Scholar]
- Ghasemiyeh P, Fazlinejad R, Kiafar MR, Rasekh S, Mokhtarzadegan M, Mohammadi-Samani S. Different therapeutic approaches in melasma: advances and limitations. Front Pharmacol 2024; 15:1337282. doi: 10.3389/fphar.2024.1337282 [Crossref] [ Google Scholar]
- Nasir A, Harikumar SL, Amanpreet K. Niosomes: an excellent tool for drug delivery. Int J Res Pharm Chem 2012; 2(2):479-87. [ Google Scholar]
- Akram MW, Jamshaid H, Rehman FU, Zaeem M, Khan JZ, Zeb A. Transfersomes: a revolutionary nanosystem for efficient transdermal drug delivery. AAPS PharmSciTech 2021; 23(1):7. doi: 10.1208/s12249-021-02166-9 [Crossref] [ Google Scholar]
- Kheirieh A, Kheirieh A, Mahdavi Z, Halvani AM, Bagheri AM, Nassirli H. Energy-based methods and nanocarrier-based approaches for melasma treatment. Adv Pharm Bull 2024; 14(4):759-93. doi: 10.34172/apb.42794 [Crossref] [ Google Scholar]
- Alharbi WS, Almughem FA, Almehmady AM, Jarallah SJ, Alsharif WK, Alzahrani NM. Phytosomes as an emerging nanotechnology platform for the topical delivery of bioactive phytochemicals. Pharmaceutics 2021; 13(9):1475. doi: 10.3390/pharmaceutics13091475 [Crossref] [ Google Scholar]
- Lu M, Qiu Q, Luo X, Liu X, Sun J, Wang C. Phyto-phospholipid complexes (phytosomes): a novel strategy to improve the bioavailability of active constituents. Asian J Pharm Sci 2019; 14(3):265-74. doi: 10.1016/j.ajps.2018.05.011 [Crossref] [ Google Scholar]
- Obiedallah MM, Mironov MA, Belyaev DV, Ene A, Vakhrusheva DV, Krasnoborova SY. Optimization, characterization, and cytotoxicity studies of novel anti-tubercular agent-loaded liposomal vesicles. Sci Rep 2024; 14(1):524. doi: 10.1038/s41598-023-49576-2 [Crossref] [ Google Scholar]
- Nguyen VD, Zheng S, Han J, Le VH, Park JO, Park S. Nanohybrid magnetic liposome functionalized with hyaluronic acid for enhanced cellular uptake and near-infrared-triggered drug release. Colloids Surf B Biointerfaces 2017; 154:104-14. doi: 10.1016/j.colsurfb.2017.03.008 [Crossref] [ Google Scholar]
- Sinico C, Fadda AM. Vesicular carriers for dermal drug delivery. Expert Opin Drug Deliv 2009; 6(8):813-25. doi: 10.1517/17425240903071029 [Crossref] [ Google Scholar]
- Kirjavainen M, Urtti A, Jääskeläinen I, Suhonen TM, Paronen P, Valjakka-Koskela R. Interaction of liposomes with human skin in vitro--the influence of lipid composition and structure. Biochim Biophys Acta 1996; 1304(3):179-89. doi: 10.1016/s0005-2760(96)00126-9 [Crossref] [ Google Scholar]
- El Maghraby GM, Williams AC, Barry BW. Skin delivery of oestradiol from deformable and traditional liposomes: mechanistic studies. J Pharm Pharmacol 1999; 51(10):1123-34. doi: 10.1211/0022357991776813 [Crossref] [ Google Scholar]
- Ahmad A, Ahsan H. Lipid-based formulations in cosmeceuticals and biopharmaceuticals. Biomed Dermatol 2020; 4(1):12. doi: 10.1186/s41702-020-00062-9 [Crossref] [ Google Scholar]
- Soni V, Chandel S, Jain P, Asati S. Role of liposomal drug-delivery system in cosmetics. In: Grumezescu AM, ed. Nanobiomaterials in Galenic Formulations and Cosmetics. William Andrew Publishing; 2016. p. 93-120. doi: 10.1016/b978-0-323-42868-2.00005-x.
- Ahmadi Ashtiani H, Bishe P, Lashgari N, Nilforoushzadeh MA, Zare S. Liposomes in cosmetics. J Skin Stem Cell 2016; 3(3):e65815. doi: 10.5812/jssc.65815 [Crossref] [ Google Scholar]
- Choo W, Tey HL. Skin lightening efficacy of tranexamic acid in topical delivery systems. Clin Exp Dermatol Ther 2023; 9:229. doi: 10.29011/2575-8268.100229 [Crossref] [ Google Scholar]
- Manosroi A, Podjanasoonthon K, Manosroi J. Development of novel topical tranexamic acid liposome formulations. Int J Pharm 2002; 235(1-2):61-70. doi: 10.1016/s0378-5173(01)00980-2 [Crossref] [ Google Scholar]
- Manosroi A, Podjanasoonthon K, Manosroi J. Stability and release of topical tranexamic acid liposome formulations. J Cosmet Sci 2002; 53(6):375-86. [ Google Scholar]
- Banihashemi M, Zabolinejad N, Jaafari MR, Salehi M, Jabari A. Comparison of therapeutic effects of liposomal tranexamic acid and conventional hydroquinone on melasma. J Cosmet Dermatol 2015; 14(3):174-7. doi: 10.1111/jocd.12152 [Crossref] [ Google Scholar]
- Xing X, Chen L, Xu Z, Jin S, Zhang C, Xiang L. The efficacy and safety of topical tranexamic acid (liposomal or lotion with microneedling) versus conventional hydroquinone in the treatment of melasma. J Cosmet Dermatol 2020; 19(12):3238-44. doi: 10.1111/jocd.13810 [Crossref] [ Google Scholar]
- Manfreda V, Eleonora DM, Luca B. Efficacy and safety of Politranexamide® liposomal emulsion on facial melasma: a comparative study. J Cosmet Dermatol 2023; 22(6):1780-5. doi: 10.1111/jocd.15648 [Crossref] [ Google Scholar]
- Fahr A, Chen M. Liposomes as promising tools for the skin delivery and protection of damaged skin. In: Toxicology of the Skin. CRC Press; 2010. p. 303-14.
- Morrow DI, McCarron PA, Woolfson AD, Donnelly RF. Innovative strategies for enhancing topical and transdermal drug delivery. Open Drug Deliv J 2007; 107(1):36-59. doi: 10.2174/1874126600701010036 [Crossref] [ Google Scholar]
- Roberts MS, Mohammed Y, Pastore MN, Namjoshi S, Yousef S, Alinaghi A. Topical and cutaneous delivery using nanosystems. J Control Release 2017; 247:86-105. doi: 10.1016/j.jconrel.2016.12.022 [Crossref] [ Google Scholar]
- Verma P, Pathak K. Therapeutic and cosmeceutical potential of ethosomes: an overview. J Adv Pharm Technol Res 2010; 1(3):274-82. doi: 10.4103/0110-5558.72415 [Crossref] [ Google Scholar]
- Alshehri S, Hussain A, Altamimi MA, Ramzan M. In vitro, ex vivo, and in vivo studies of binary ethosomes for transdermal delivery of acyclovir: a comparative assessment. J Drug Deliv Sci Technol 2021; 62:102390. doi: 10.1016/j.jddst.2021.102390 [Crossref] [ Google Scholar]
- Pandey V, Golhani D, Shukla R. Ethosomes: versatile vesicular carriers for efficient transdermal delivery of therapeutic agents. Drug Deliv 2015; 22(8):988-1002. doi: 10.3109/10717544.2014.889777 [Crossref] [ Google Scholar]
- Yu X, Du L, Li Y, Fu G, Jin Y. Improved anti-melanoma effect of a transdermal mitoxantrone ethosome gel. Biomed Pharmacother 2015; 73:6-11. doi: 10.1016/j.biopha.2015.05.002 [Crossref] [ Google Scholar]
- Paiva-Santos AC, Silva AL, Guerra C, Peixoto D, Pereira-Silva M, Zeinali M. Ethosomes as nanocarriers for the development of skin delivery formulations. Pharm Res 2021; 38(6):947-70. doi: 10.1007/s11095-021-03053-5 [Crossref] [ Google Scholar]
- Mehmood Y, Shahid H, Ahmed S, Khursheed A, Jamshaid T, Jamshaid M. Synthesis of vitamin D3 loaded ethosomes gel to cure chronic immune-mediated inflammatory skin disease: physical characterization, in vitro and ex vivo studies. Sci Rep 2024; 14(1):23866. doi: 10.1038/s41598-024-72951-6 [Crossref] [ Google Scholar]
- Chauhan M, Chandra J, Gupta G, Ramaiah R, Hani U, Kesharwani P. Harnessing phytoconstituents in ethosomes: a new frontier in skin disorder management. Int J Pharm 2025; 671:125273. doi: 10.1016/j.ijpharm.2025.125273 [Crossref] [ Google Scholar]
- Zhan B, Wang J, Li H, Xiao K, Fang X, Shi Y. Ethosomes: a promising drug delivery platform for transdermal application. Chemistry 2024; 6(5):993-1019. doi: 10.3390/chemistry6050058 [Crossref] [ Google Scholar]
- Niu XQ, Zhang DP, Bian Q, Feng XF, Li H, Rao YF. Mechanism investigation of ethosomes transdermal permeation. Int J Pharm X 2019; 1:100027. doi: 10.1016/j.ijpx.2019.100027 [Crossref] [ Google Scholar]
- Noh TK, Choi SJ, Chung BY, Kang JS, Lee JH, Lee MW. Inflammatory features of melasma lesions in Asian skin. J Dermatol 2014; 41(9):788-94. doi: 10.1111/1346-8138.12573 [Crossref] [ Google Scholar]
- Shaji J, Parab SS. Formulation development of tranexamic acid loaded transethosomal patch for melasma. Research Journal of Pharmaceutical Dosage Forms and Technology 2022; 14:7-16. doi: 10.52711/0975-4377.2022.00002 [Crossref] [ Google Scholar]
- Chowdary P, Padmakumar A, Rengan AK. Exploring the potential of transethosomes in therapeutic delivery: a comprehensive review. MedComm Biomater Appl 2023; 2(4):e59. doi: 10.1002/mba2.59 [Crossref] [ Google Scholar]
- Celia C, Cilurzo F, Trapasso E, Cosco D, Fresta M, Paolino D. Ethosomes® and transfersomes® containing linoleic acid: physicochemical and technological features of topical drug delivery carriers for the potential treatment of melasma disorders. Biomed Microdevices 2012; 14(1):119-30. doi: 10.1007/s10544-011-9590-y [Crossref] [ Google Scholar]
- Tanveer N, Khan HM, Akhtar N. Whitening effect of kojic acid dipalmitate loaded nanosized ethosomal gel for the treatment of hyperpigmentation: in vitro and in vivo characterization. J Cosmet Dermatol 2022; 21(12):6850-62. doi: 10.1111/jocd.15408 [Crossref] [ Google Scholar]
- Grossi LN, Braz WR, da Silva NP, Cazarim EL, Palmieri MG, Tavares GD. Ethosomes as delivery system for treatment of melanoma: a mini-review. Oncologie 2023; 25(5):455-9. doi: 10.1515/oncologie-2023-0177 [Crossref] [ Google Scholar]
- Pooprommin P, Manaspon C, Dwivedi A, Mazumder A, Sangkaew S, Wanmasae S. Alginate/pectin dressing with niosomal mangosteen extract for enhanced wound healing: evaluating skin irritation by structure-activity relationship. Heliyon 2022; 8(12):e12032. doi: 10.1016/j.heliyon.2022.e12032 [Crossref] [ Google Scholar]
- Namdeo A, Jain NK. Niosomes as drug carriers. Indian J Pharm Sci 1996; 58(2):41-6. [ Google Scholar]
- Bartelds R, Nematollahi MH, Pols T, Stuart MCA, Pardakhty A, Asadikaram G. Niosomes, an alternative for liposomal delivery. PLoS One 2018; 13(4):e0194179. doi: 10.1371/journal.pone.0194179 [Crossref] [ Google Scholar]
- Kazi KM, Mandal AS, Biswas N, Guha A, Chatterjee S, Behera M. Niosome: a future of targeted drug delivery systems. J Adv Pharm Technol Res 2010; 1(4):374-80. doi: 10.4103/0110-5558.76435 [Crossref] [ Google Scholar]
- Mujoriya R, Bodla RB, Dhamande K, Singh D, Patle L. Niosomal drug delivery system: the magic bullet. J Appl Pharm Sci 2011; 1(9):20-3. [ Google Scholar]
- Mujoriya RZ, Bodla R. Niosomes–challenge in preparation for pharmaceutical scientist. Int J Appl Pharm 2011; 3(3):11-5. [ Google Scholar]
- Sankhyan A, Pawar P. Recent trends in niosome as vesicular drug delivery system. J Appl Pharm Sci 2012; 2(6):20-32. doi: 10.7324/japs.2012.2625 [Crossref] [ Google Scholar]
- Mawazi SM, Ann TJ, Widodo RT. Application of niosomes in cosmetics: a systematic review. Cosmetics 2022; 9(6):127. doi: 10.3390/cosmetics9060127 [Crossref] [ Google Scholar]
- Wu X, Guy RH. Applications of nanoparticles in topical drug delivery and in cosmetics. J Drug Deliv Sci Technol 2009; 19(6):371-84. doi: 10.1016/s1773-2247(09)50080-9 [Crossref] [ Google Scholar]
- Bugaj AM. Intradermal delivery of active cosmeceutical ingredients. In: Novel Delivery Systems for Transdermal and Intradermal Drug Delivery. John Wiley & Sons; 2015. p. 209-42. doi: 10.1002/9781118734506.ch10.
- Sharma B, Sharma A. Future prospect of nanotechnology in development of anti-ageing formulations. Int J Pharm Pharm Sci 2012; 4(3):57-66. [ Google Scholar]
- Kesharwani P, Dubey SK. Nanocosmetics: Delivery Approaches, Applications and Regulatory Aspects. Boca Raton: CRC Press; 2023. doi: 10.1201/9781003319146.
- Salvioni L, Morelli L, Ochoa E, Labra M, Fiandra L, Palugan L. The emerging role of nanotechnology in skincare. Adv Colloid Interface Sci 2021; 293:102437. doi: 10.1016/j.cis.2021.102437 [Crossref] [ Google Scholar]
- Oliveira C, Coelho C, Teixeira JA, Ferreira-Santos P, Botelho CM. Nanocarriers as active ingredients enhancers in the cosmetic industry-the European and North America regulation challenges. Molecules 2022; 27(5):1669. doi: 10.3390/molecules27051669 [Crossref] [ Google Scholar]
- Singh TG, Sharma N. Nanobiomaterials in cosmetics: current status and future prospects. In: Grumezescu AM, ed. Nanobiomaterials in Galenic Formulations and Cosmetics. William Andrew Publishing; 2016. p. 149-74. doi: 10.1016/b978-0-323-42868-2.00007-3.
- Shatalebi MA, Mostafavi SA, Moghaddas A. Niosome as a drug carrier for topical delivery of N-acetyl glucosamine. Res Pharm Sci 2010; 5(2):107-17. [ Google Scholar]
- Ammar AA, Salem HA, Eladawy SA, Elsamad Z, Kohaf NA. Development and clinical evaluation of topical hydroquinone niosomal gel formulation for the treatment of melasma. Int J App Pharm 2020; 12(4):228-36. doi: 10.22159/ijap.2020v12i4.34304 [Crossref] [ Google Scholar]
- Divanbeygikermani M, Pardakhty A, Amanatfard A. Kojic acid and hydroquinone non-ionic surfactant vesicles for topical application. Int Pharm Acta 2018; 1(1):110. doi: 10.22037/ipa.v1i1.20494 [Crossref] [ Google Scholar]
- Lu B, Huang Y, Chen Z, Ye J, Xu H, Chen W. Niosomal Nanocarriers for enhanced skin delivery of quercetin with functions of anti-tyrosinase and antioxidant. Molecules 2019; 24(12):2322. doi: 10.3390/molecules24122322 [Crossref] [ Google Scholar]
- Manosroi A, Chutoprapat R, Abe M, Manosroi W, Manosroi J. Anti-aging efficacy of topical formulations containing niosomes entrapped with rice bran bioactive compounds. Pharm Biol 2012; 50(2):208-24. doi: 10.3109/13880209.2011.596206 [Crossref] [ Google Scholar]
- Ricci A, Stefanuto L, Gasperi T, Bruni F, Tofani D. Lipid nanovesicles for antioxidant delivery in skin: liposomes, ufasomes, ethosomes, and niosomes. Antioxidants (Basel) 2024; 13(12):1516. doi: 10.3390/antiox13121516 [Crossref] [ Google Scholar]
- Uma M, Nagaraja TS, Vijapure VK, Bharathi DR. Development and evaluation of niosomal drug delivery system containing tranexamic acid. Indo Am J Pharm Sci 2019; 6(6):13113-223. doi: 10.5281/zenodo.3257978 [Crossref] [ Google Scholar]
- Wadher K, Trivedi S, Rarokar N, Umekar M. Development and assessment of rutin loaded transfersomes to improve ex vivo membrane permeability and in vitro efficacy. Hybrid Adv 2024; 5:100144. doi: 10.1016/j.hybadv.2024.100144 [Crossref] [ Google Scholar]
- Li J, Duan N, Song S, Nie D, Yu M, Wang J. Transfersomes improved delivery of ascorbic palmitate into the viable epidermis for enhanced treatment of melasma. Int J Pharm 2021; 608:121059. doi: 10.1016/j.ijpharm.2021.121059 [Crossref] [ Google Scholar]
- Lee MH, Lee KK, Park MH, Hyun SS, Kahn SY, Joo KS. In vivo anti-melanogenesis activity and in vitro skin permeability of niacinamide-loaded flexible liposomes (BounsphereTM). J Drug Deliv Sci Technol 2016; 31:147-52. doi: 10.1016/j.jddst.2015.12.008 [Crossref] [ Google Scholar]
- Barani M, Sangiovanni E, Angarano M, Rajizadeh MA, Mehrabani M, Piazza S. Phytosomes as innovative delivery systems for phytochemicals: a comprehensive review of literature. Int J Nanomedicine 2021; 16:6983-7022. doi: 10.2147/ijn.S318416 [Crossref] [ Google Scholar]
- Dwivedi D, Shukla AK, Singh SP. Phytosomes: an emerging approach for effective management of dermatological disorder. Int J Res Pharm Sci 2022; 13(1):8-14. doi: 10.26452/ijrps.v13i1.11 [Crossref] [ Google Scholar]
- Priani SE, Aprilia S, Aryani R, Purwanti L. Antioxidant and tyrosinase inhibitory activity of face serum containing cocoa pod husk phytosome (Theobroma cacao L). J Appl Pharm Sci 2019; 9(10):110-5. doi: 10.7324/japs.2019.91015 [Crossref] [ Google Scholar]
- Patel RK, Jadeja MB. Development and evaluation of phosphatidylcholine complexes of arbutin as skin whitening agent. Int J Pharm Sci Res 2021; 12(2):917-27. doi: 10.13040/ijpsr.0975-8232.12(2).917-27 [Crossref] [ Google Scholar]
- Permana AD, Utami RN, Courtenay AJ, Manggau MA, Donnelly RF, Rahman L. Phytosomal nanocarriers as platforms for improved delivery of natural antioxidant and photoprotective compounds in propolis: an approach for enhanced both dissolution behaviour in biorelevant media and skin retention profiles. J Photochem Photobiol B 2020; 205:111846. doi: 10.1016/j.jphotobiol.2020.111846 [Crossref] [ Google Scholar]
- Pan X, Zhong Z, Hu X, Wu J, Huang W, Li W, et al. Application of nanotechnology in anti-aging cosmetics: advantages, challenges, and prospects. Polym Bull 2025. doi: 10.1007/s00289-025-05903-3.
- Abu-Huwaij R, Zidan AN. Unlocking the potential of cosmetic dermal delivery with ethosomes: a comprehensive review. J Cosmet Dermatol 2024; 23(1):17-26. doi: 10.1111/jocd.15895 [Crossref] [ Google Scholar]
- Parać E, Bukvić Mokos Z. Unmasking melasma: confronting the treatment challenges. Cosmetics 2024; 11(4):143. doi: 10.3390/cosmetics11040143 [Crossref] [ Google Scholar]
- Gaspar RS, Silva-Lima B, Magro F, Alcobia A, da Costa FL, Feio J. Non-biological complex drugs (NBCDs): complex pharmaceuticals in need of individual robust clinical assessment before any therapeutic equivalence decision. Front Med (Lausanne) 2020; 7:590527. doi: 10.3389/fmed.2020.590527 [Crossref] [ Google Scholar]
- Wang Y, Grainger DW. Regulatory considerations specific to liposome drug development as complex drug products. Front Drug Deliv 2022; 2:901281. doi: 10.3389/fddev.2022.901281 [Crossref] [ Google Scholar]
- US Food and Drug Administration. Considering Whether an FDA-Regulated Product Involves the Application of Nanotechnology. FDA; 2014. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/considering-whether-fda-regulated-product-involves-application-nanotechnology.