Advanced pharmaceutical bulletin. 15(4):939-947.
doi: 10.34172/apb.025.46028
Original Article
Investigating the Role of Empagliflozin in the Pathological Progress of Ischemia-Reperfusion Injury in Rat Kidneys: The Involvement of Nitric Oxide
Amin Hasanvand Conceptualization, Investigation, Methodology, Project administration, Validation, Writing – original draft, 1 
Abdolreza Tajdar Investigation, 2
Azita Zafar Mohtashami Investigation, 3
Zahra Haghighatian Investigation, 4
Elham Goodarzi Data curation, Formal analysis, Visualization, 5
Peyman Amanolahi Baharvand Supervision, Validation, Writing – original draft, Writing – review & editing, 6
Babak Hadian Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – review & editing, 3, *
Author information:
1Department of Physiology and Pharmacology, School of Medicine, Lorestan University of Medical Sciences, Khorramabad, Iran
2Student Research Committee, Lorestan University of Medical Sciences, Khorramabad, Iran
3Department of Nephrology, Faculty of Medicine, Lorestan University of Medical Sciences, Khorramabad, Iran
4Department of Pathology, School of Medicine, Lorestan University of Medical Science, Khorramabad, Iran
5Department of Biostatistics and Epidemiology, School of Health and Nutrition, Lorestan University of Medical Sciences, Khorramabad, Iran
6Department of English, School of Medicine, AJA University of Medical Sciences, Tehran, Iran
Abstract
Purpose:
Renal ischemia-reperfusion (RIR) is a pathological condition that can lead to severe outcomes due to damage to kidney structures. Additionally, oxidative stress is triggered by mitochondrial disruption during reperfusion, potentially resulting in necrosis and, ultimately, cell death through the destruction of cellular membranes.
Methods:
Thirty rats were included in this study and divided into the following groups: healthy rats, an ischemia-reperfusion (I/R) group, an I/R group treated with empagliflozin, an I/R group treated with empagliflozin plus L-NAME, and an I/R group treated with empagliflozin plus L-arginine. The drugs were administered from three days before I/R induction to one day post-operation. Blood samples were collected 24 hours after I/R induction to evaluate renal function, inflammatory markers, and oxidative stress. Subsequently, the right kidney was harvested for nitric oxide (NO) measurement, while the left kidney was used for histological analysis.
Results:
Empagliflozin administration significantly reduced creatinine, urea, inflammatory markers, and oxidative stress levels. Moreover, empagliflozin increased the levels of antioxidant enzymes and NO. Histopathological analysis indicated that empagliflozin mitigated ischemia-reperfusion injury in renal tissue. The protective effects were further enhanced with the co-administration of empagliflozin and L-arginine. In contrast, simultaneous treatment with empagliflozin and L-NAME led to pathological changes associated with ischemia-reperfusion and attenuated the beneficial effects of empagliflozin.
Conclusion:
The findings of this study suggest that empagliflozin exerts protective effects against ischemia-reperfusion injury, likely through the NO pathway.
Keywords: Renal, Ischemia-reperfusion, Empagliflozin, Nitric oxide, Rat
Copyright and License Information
© 2025 The Author (s).
This is an Open Access article distributed under the terms of the Creative Commons Attribution (CC BY), which permits unrestricted use, distribution, and reproduction in any medium, as long as the original authors and source are cited. No permission is required from the authors or the publishers.
Funding Statement
This study was financially supported by Lorestan University of Medical Sciences.
Introduction
Renal ischemia-reperfusion (RIR) is a critical pathological condition that causes structural and functional damage to the kidneys.1 During renal ischemia, anaerobic conditions reduce ATP production, leading to cell membrane damage, cellular swelling, and activation of inflammatory pathways.2 Renal reperfusion elevates oxidative stress, leading to mitochondrial dysfunction, cell membrane damage, and necrotic cell death.2 Numerous studies indicate that inflammatory cytokines and oxidative stress during reperfusion significantly contribute to renal injury and tubular damage.3,4 Renal proximal tubular epithelial cells are highly susceptible to ischemia, and hypoxia can compromise nephron structural integrity.5 During renal reperfusion, the S3 segment of proximal tubules undergoes apoptosis and necrosis, potentially resulting in renal dysfunction.6 Nitric oxide is one of the most important vasodilator enzymes and plays a central role in the regulation of renal hemodynamics.7 Reduced nitric oxide (NO) production in the kidneys may contribute to the progression of chronic kidney disease.8,9 Studies have also shown that kidney tissue nitrite levels are significantly reduced during ischemia-reperfusion.10,11 Studies show that NO protects the kidneys by enhancing ATP synthesis, inhibiting apoptosis, and reducing inflammatory cytokine activity.12 It may also lower the risk of acute kidney injury in patients undergoing cardiopulmonary bypass surgery.13 Empagliflozin, a sodium-glucose cotransporter-2 (SGLT2) inhibitor, promotes renal glucose excretion and demonstrates renoprotective effects in various models.14 Chang Chu et al. found that empagliflozin reduced kidney injury molecule-1 expression and restored normal miR-26a levels in an ischemia-reperfusion model.15 Additionally, empagliflozin can reduce intraglomerular pressure, lower the risk of end-stage renal disease, improve kidney filtration, and enhance renal function.16,17 It exerts protective effects by increasing GSK-3β phosphorylation during renal ischemia-reperfusion and by activating the AMPK–OPA1 signaling pathway.18,19 Several studies have also shown that empagliflozin increases NO activity and bioavailability, contributing to its renal protective effects.20,21 Given the role of NO in kidney protection and its stimulation by empagliflozin, we evaluated empagliflozin’s effects on the NO signaling pathway in this study. We further assessed its impact on renal structure, tissue nitrite levels, inflammatory cytokines, and oxidative stress during renal ischemia-reperfusion.
Materials and Methods
Animals and group descriptions
In this experimental study, thirty male Wistar rats weighing 160–180 g were used. During the study, the animals were maintained under controlled conditions at 21–25 °C with a 12-hour light/dark cycle and housed in standard polyethylene cages. Empagliflozin (Actoverco, Tehran, Iran), L-arginine (Merck KGaA, Darmstadt, Germany), and L-NAME (Sigma-Aldrich, St. Louis, MO, USA) were used. After a two-week adaptation period to laboratory conditions, the animals were randomly allocated into five groups: Group 1, healthy rats without ischemia-reperfusion (the sham group); Group 2, ischemia-reperfusion rats (the vehicle group); Group 3, ischemia-reperfusion rats treated with empagliflozin (10 mg/kg, gavage); Group 4, ischemia-reperfusion rats treated with empagliflozin (10 mg/kg, gavage) and L-NAME (20 mg/kg, intraperitoneally); and Group 5, ischemia-reperfusion rats treated with empagliflozin (10 mg/kg, gavage) and L-arginine (200 mg/kg, intraperitoneally). The doses of empagliflozin, L-arginine, and L-NAME were selected based on previously published studies.22-25
Ischemia reperfusion induction
Three days before reperfusion ischemia induction, the drugs were administered daily until the day after surgery. To induce ischemia-reperfusion, the rats underwent a 24-hour fasting period followed by anesthesia with pentobarbital. Both kidneys were subjected to ischemia-reperfusion surgery according to the established protocol. After anesthesia, the lateral areas of the rats were shaved and disinfected. A surgical incision was made to expose the kidneys, and the renal artery was identified. Blood flow was then occluded for 45 minutes using a vascular clip to induce ischemia. Reperfusion was initiated by removing the clip, and the surgical site was sutured. The day after ischemia-reperfusion induction, the rats were re-anesthetized for cardiac blood collection. Both kidneys were harvested for pathological examination and NO measurement. Finally, the animals were euthanized with ether according to established guidelines.26
Assessment of kidney biomarkers
After collecting blood from the heart, the samples were centrifuged to separate the serum. Serum creatinine and urea levels were then measured using commercial laboratory kits (Pars Azmoun, Iran) following the manufacturer’s instructions. These measurements were performed to assess renal function in the experimental animals.27
Assessment of oxidative stress and inflammatory enzymes levels
Blood samples collected from the heart were centrifuged at 3,500 rpm for 20 minutes to separate the serum. The supernatant was then used to measure oxidative stress markers, including malondialdehyde (MDA) and catalase (CAT), as well as inflammatory enzymes, such as TNF-alpha and CRP. All measurements were performed using commercially available ELISA kits (Abcam, USA) following the manufacturer’s protocols. These analyses were conducted to evaluate oxidative stress and inflammatory responses in the experimental animals.28
Assessment of tissue nitrite levels
The right kidney was carefully excised to determine NO concentration. For this purpose, 0.5 mL of tissue homogenate was mixed with 0.1 mL of sulfosalicylic acid and incubated for 30 minutes. The mixture was then centrifuged at 5,000 rpm for 15 minutes to obtain a protein-free supernatant, which was subsequently used for nitrite estimation. A volume of 30 μL of 10% NaOH was added to 200 μL of the supernatant, followed by 300 μL of Tris-HCl buffer, and the solution was thoroughly mixed. Thereafter, 530 μL of Griess reagent was added, and the mixture was incubated in the dark for 10–15 minutes. Absorbance was measured at 540 nm against a Griess reagent blank. Sodium nitrite solution was employed as the standard, and nitrite concentrations in the samples were calculated using standard calibration curves.29
Histopathology
The left kidney was carefully excised for histopathological examination. Samples were fixed in 10% buffered formalin and processed using a tissue processor. Sequential procedures, including tissue dehydration, embedding, sectioning, and hematoxylin-eosin staining, were performed in the pathology laboratory. To ensure blinding, all slides were numerically coded prior to assessment. Histological evaluation was conducted by a blinded pathologist according to predefined criteria for inflammation, tubular injury, and glomerular alterations. The kidney samples were specifically examined for inflammation, renal tubular dilation, glomerular mesangial proliferation, hemorrhage, and tubular degeneration.30 Histopathological images were acquired using Leica microscope imaging software.
Statistical analysis
Data are presented as mean ± standard deviation (SD) and analyzed using PRISM software. Before performing parametric analyses, normality and homogeneity of variances were assessed using the Shapiro–Wilk and Levene’s tests, respectively. One-way ANOVA was then applied, followed by Tukey’s post-hoc test for multiple comparisons. A P value of less than 0.05 was considered statistically significant.
Results
Evaluation of creatinine levels
As shown in Table 1, rats subjected to ischemia-reperfusion exhibited a significant increase in creatinine levels compared with the healthy (sham) group (P< 0.001). Administration of empagliflozin alone (group 3) or in combination with L-arginine (group 5) significantly reduced creatinine levels compared with the ischemia-reperfusion vehicle group (group 2) (P < 0.001). Group 4, which received empagliflozin with L-NAME, also showed a reduction in creatinine levels compared with group 2, but this difference was less pronounced (P < 0.05).
Table 1.
Serum creatinine and urea levels in different experimental groups following ischemia-reperfusion (I/R) injury and treatment with empagliflozin and nitric oxide modulators
|
Biochemical parameters
|
Groups
|
|
Healthy Animals
|
I/RGroup
|
I/R Group+Empagliflozin
|
I/R Group+L-NAME
|
I/R Group+L-Arginine
|
| Creatinine (mg/dL) |
0.57 |
1.51&&& |
1.03&&&/*** |
1.19&&&/* |
0.87&/***/@@ |
| Urea (mg/dL) |
34.69 |
79.42&&& |
65.71&&&/* |
72.67&&& |
49.52&&/***/$$/@@@ |
Data represent the mean values from six animals per group. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P < 0.01, ***P < 0.001 compared with the ischemia/reperfusion group. $P < 0.05, $$P < 0.01, $$$P < 0.001 compared with the empagliflozin group. @P < 0.05, @@P < 0.01, @@@P < 0.001 compared with the group receiving empagliflozin and L.NAME. IR significantly increased serum creatinine and urea levels compared with healthy controls. Treatment with empagliflozin reduced both parameters, indicating renal protection. Co-administration of empagliflozin with L-arginine further improved renal function, showing the lowest creatinine and urea values. In contrast, co-administration with L-NAME (a nitric oxide synthase inhibitor) attenuated the protective effects of empagliflozin.
Evaluation of urea levels
As shown in Table 1, rats subjected to ischemia-reperfusion exhibited significantly higher urea levels compared with the healthy (sham) group (P < 0.001). Administration of empagliflozin alone (group 3, P < 0.05) or in combination with L-arginine (group 5, P < 0.001) significantly reduced urea levels compared with the ischemia-reperfusion vehicle group (group 2). No significant change was observed in group 4 (empagliflozin + L-NAME) compared with group 2. Notably, urea levels in group 5 were significantly lower than in group 3 (P < 0.01), whereas groups receiving L-NAME did not differ significantly from group 3. Finally, a significant difference was observed between the L-NAME and L-arginine groups (P < 0.001).
Evaluation of TNF-α and CRP enzyme levels
As shown in Figures 1A and 1B, inflammatory cytokine levels were significantly elevated in the ischemia-reperfusion vehicle group (group 2) compared with the healthy (sham) group (group 1). Administration of empagliflozin (group 3) significantly reduced these cytokine levels (P < 0.001). In group 4, inhibition of NO synthesis led to a moderate but significant decrease in inflammatory cytokines compared with group 2 (P < 0.05). Notably, stimulation of the NO pathway further enhanced the reduction of inflammatory cytokines in group 5 (P< 0.001).
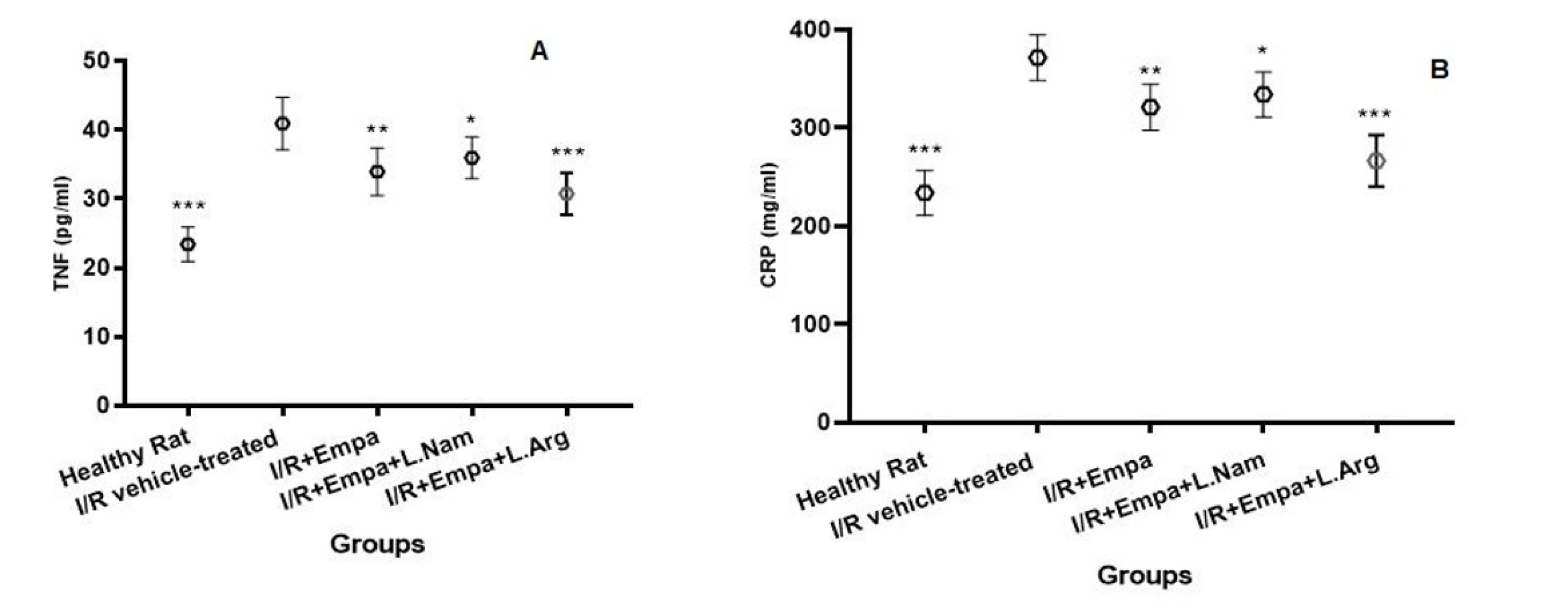
Figure 1.
Tumor necrosis factor-alpha (TNF-α, panel A) and C-reactive protein (CRP, panel B) levels in serum following ischemia-reperfusion injury and treatment with empagliflozin and nitric oxide modulators. Cytokine levels were measured in six rats per group. Data are expressed as mean ± SD. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P < 0.01, ***P < 0.001 vs. IR vehicle-treated group. IR significantly increased TNF-α and CRP levels compared with healthy controls. Empagliflozin treatment reduced both TNF-α and CRP concentrations. Co-administration of empagliflozin with L-arginine enhanced these protective effects, whereas co-administration with L-NAME partially counteracted them. Abbreviations: ischemia-reperfusion, I/R; Empa, empagliflozin; L.Nam, L-NAME; L.Arg, L-arginine
.
Tumor necrosis factor-alpha (TNF-α, panel A) and C-reactive protein (CRP, panel B) levels in serum following ischemia-reperfusion injury and treatment with empagliflozin and nitric oxide modulators. Cytokine levels were measured in six rats per group. Data are expressed as mean ± SD. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P < 0.01, ***P < 0.001 vs. IR vehicle-treated group. IR significantly increased TNF-α and CRP levels compared with healthy controls. Empagliflozin treatment reduced both TNF-α and CRP concentrations. Co-administration of empagliflozin with L-arginine enhanced these protective effects, whereas co-administration with L-NAME partially counteracted them. Abbreviations: ischemia-reperfusion, I/R; Empa, empagliflozin; L.Nam, L-NAME; L.Arg, L-arginine
Evaluation of catalase and MDA enzyme levels
As shown in Figure 2, ischemia-reperfusion induction in the vehicle group (group 2) resulted in a decrease in catalase (CAT) activity and an increase in malondialdehyde (MDA) levels. Administration of empagliflozin (group 3) significantly increased CAT activity (P < 0.05) and reduced MDA levels (P < 0.01). Co-administration of empagliflozin with L-NAME (group 4) did not significantly affect CAT activity compared with group 2, although MDA levels were moderately reduced (P < 0.05). Notably, simultaneous administration of empagliflozin and L-arginine (group 5) significantly increased CAT activity (P < 0.01) and markedly decreased MDA levels (P < 0.001).
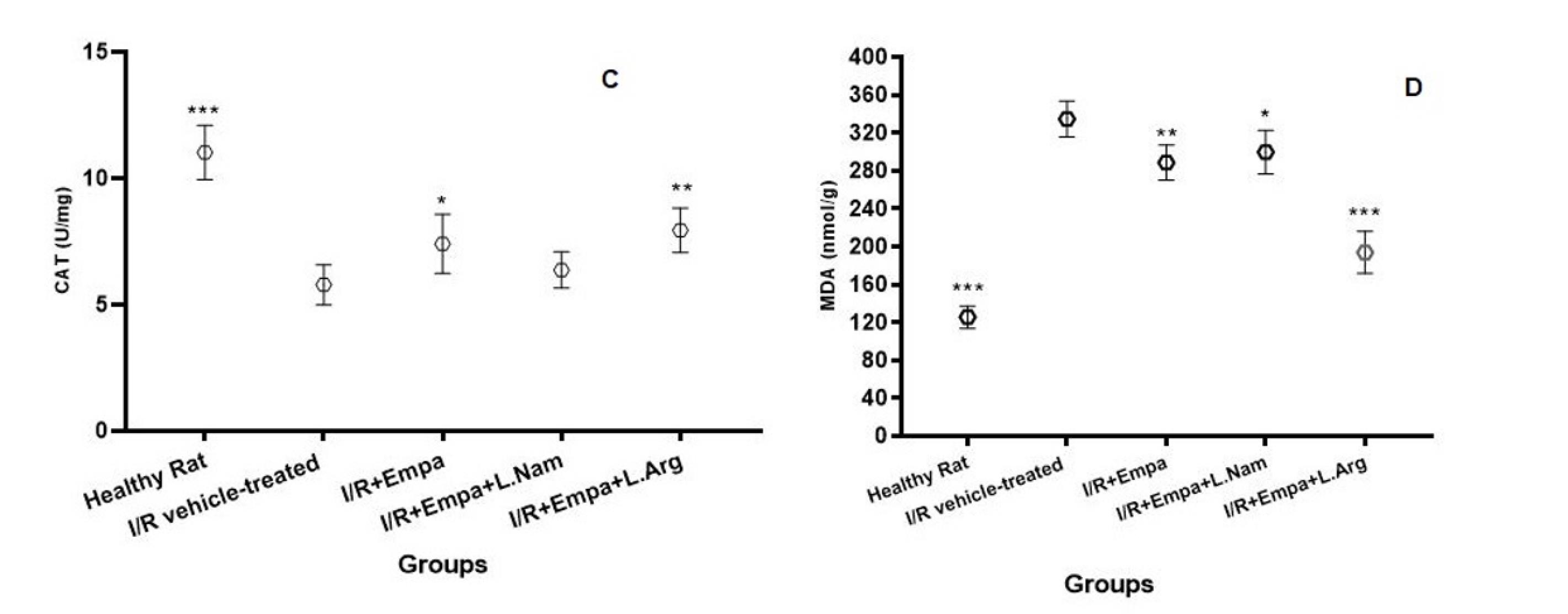
Figure 2.
Catalase (CAT, panel C) and malondialdehyde (MDA, panel D) levels in kidney tissue following ischemia-reperfusion injury and treatment with empagliflozin and nitric oxide modulators. Enzyme levels were measured in kidneys of six rats per group. Data are presented as mean ± SD. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P < 0.01, ***P < 0.001 vs. IR vehicle-treated group. IR significantly decreased CAT activity and increased MDA levels compared with healthy controls. Treatment with empagliflozin partially restored CAT activity and reduced MDA levels. Co-administration of empagliflozin with L-arginine further improved these effects, while co-administration with L-NAME attenuated the protective effects of empagliflozin. Abbreviations: ischemia-reperfusion, I/R; Empa, empagliflozin; L.Nam, L-NAME; L.Arg, L-arginine
.
Catalase (CAT, panel C) and malondialdehyde (MDA, panel D) levels in kidney tissue following ischemia-reperfusion injury and treatment with empagliflozin and nitric oxide modulators. Enzyme levels were measured in kidneys of six rats per group. Data are presented as mean ± SD. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P < 0.01, ***P < 0.001 vs. IR vehicle-treated group. IR significantly decreased CAT activity and increased MDA levels compared with healthy controls. Treatment with empagliflozin partially restored CAT activity and reduced MDA levels. Co-administration of empagliflozin with L-arginine further improved these effects, while co-administration with L-NAME attenuated the protective effects of empagliflozin. Abbreviations: ischemia-reperfusion, I/R; Empa, empagliflozin; L.Nam, L-NAME; L.Arg, L-arginine
Evaluation of Tissue Nitrite Levels
As shown in Figure 3, tissue nitrate levels in the kidneys were significantly reduced in the ischemia-reperfusion vehicle group (group 2) compared with the healthy (sham) group. Administration of empagliflozin (group 3) significantly increased NO levels (P < 0.01), and co-administration of empagliflozin with L-arginine (group 5) further enhanced this effect (P < 0.001). In contrast, co-administration of empagliflozin with L-NAME (group 4) resulted in decreased NO levels, which were not significantly different from those in group 2.
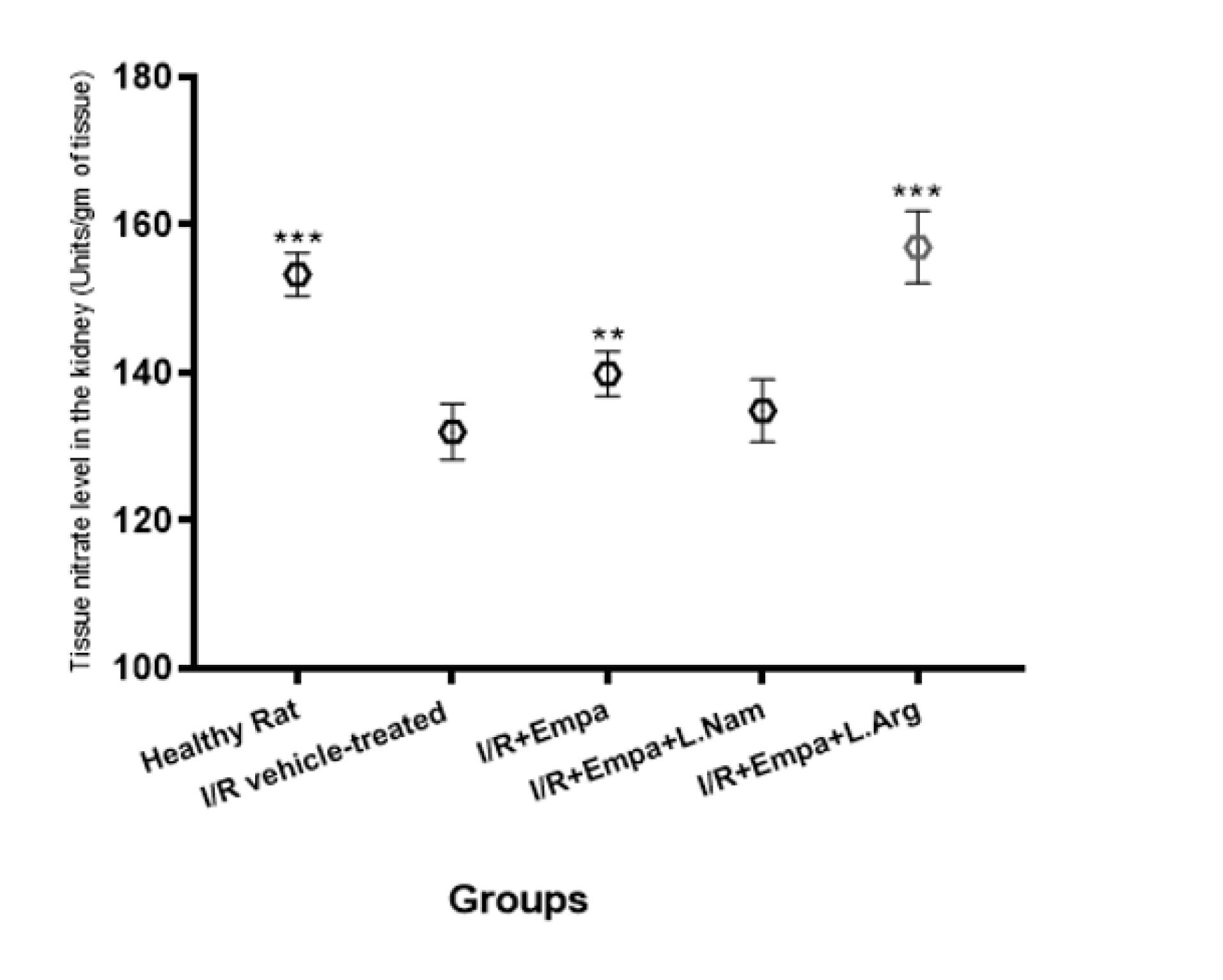
Figure 3.
Tissue nitrite levels in the kidney following ischemia-reperfusion injury and treatment with empagliflozin and nitric oxide modulators. Tissue nitrite levels were measured in kidneys of six rats per group. Data are expressed as mean ± SD. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P< 0.01, ***P < 0.001 vs. IR vehicle-treated group. IR significantly reduced tissue nitrite levels compared with healthy controls. Empagliflozin treatment alone or in combination with L-arginine significantly increased nitrite levels, while co-administration with L-NAME did not significantly alter nitrite levels compared with the IR group. Abbreviations: ischemia-reperfusion, I/R; Empa, empagliflozin; L.Nam, L-NAME; L.Arg, L-arginine
.
Tissue nitrite levels in the kidney following ischemia-reperfusion injury and treatment with empagliflozin and nitric oxide modulators. Tissue nitrite levels were measured in kidneys of six rats per group. Data are expressed as mean ± SD. Statistical analysis was performed using one-way ANOVA followed by Tukey’s post-hoc test. *P < 0.05, **P< 0.01, ***P < 0.001 vs. IR vehicle-treated group. IR significantly reduced tissue nitrite levels compared with healthy controls. Empagliflozin treatment alone or in combination with L-arginine significantly increased nitrite levels, while co-administration with L-NAME did not significantly alter nitrite levels compared with the IR group. Abbreviations: ischemia-reperfusion, I/R; Empa, empagliflozin; L.Nam, L-NAME; L.Arg, L-arginine
Histopathological Evaluation
Hematoxylin and eosin-stained kidney sections were examined, and pathological changes were scored on a semi-quantitative scale (0–4) for inflammation, tubular injury, hemorrhage, and glomerular mesenchymal proliferation. In the ischemia-reperfusion (RIR) group (Figure 4B), kidney tissues exhibited pronounced pathological alterations, with high scores for inflammation (3.5 ± 0.3), hemorrhage (3.0 ± 0.4), focal tubular injury (3.5 ± 0.2), tubular dilation and degeneration (3.0 ± 0.3), and glomerular mesenchymal proliferation (3.0 ± 0.2). Empagliflozin treatment (group 3, Figure 4C) significantly reduced these scores, indicating attenuated inflammation and tissue injury. Conversely, co-administration of empagliflozin with L-NAME (group 4, Figure 4D) resulted in worsened pathological scores, reflecting increased inflammation, hemorrhage, tubular damage, and glomerular mesenchymal proliferation. Combined treatment with empagliflozin and L-arginine (group 5, Figure 4E) significantly improved histological scores, demonstrating marked alleviation of inflammation, tubular injury, hemorrhage, and glomerular mesenchymal proliferation compared with the RIR group.
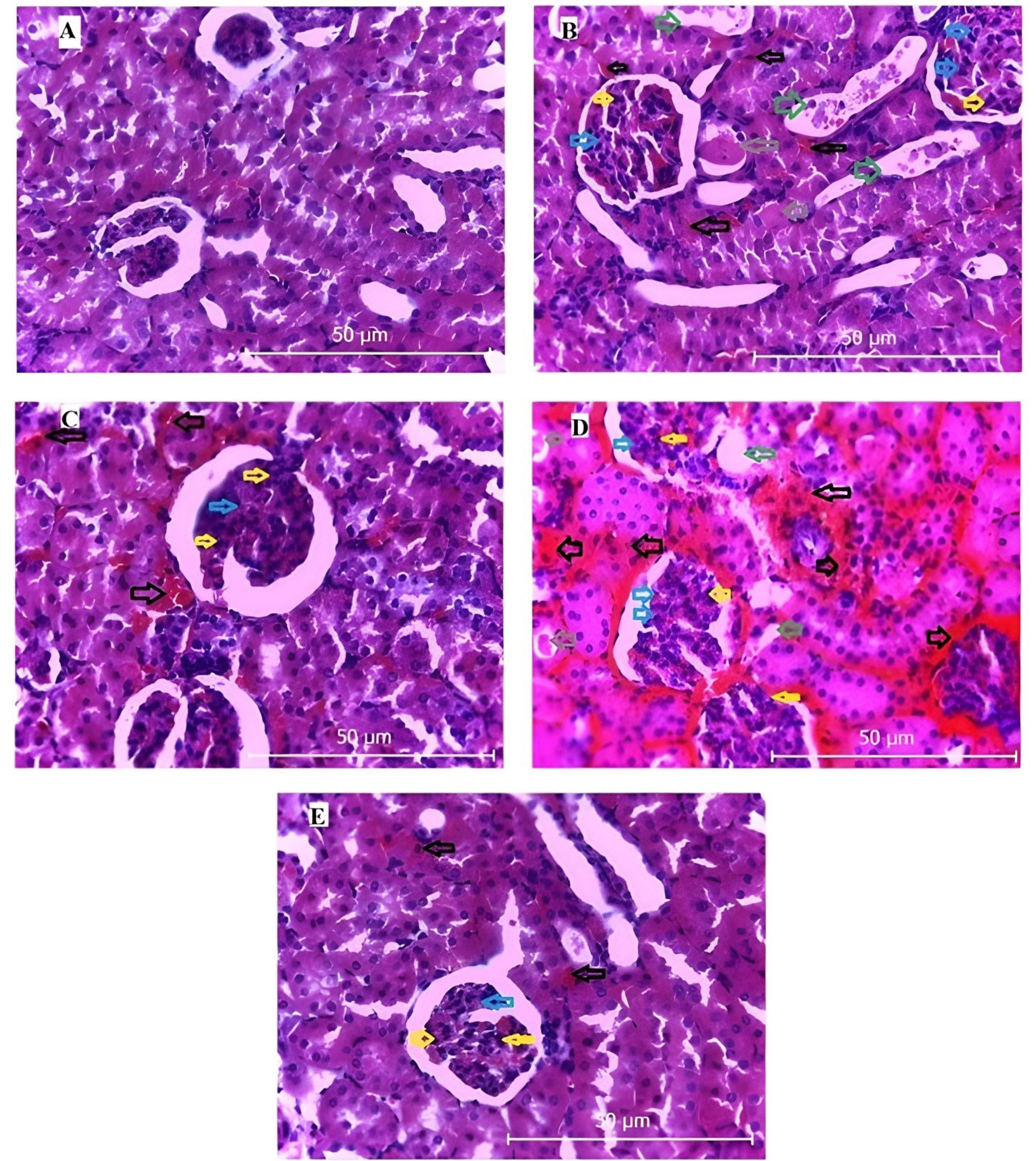
Figure 4.
Renal histopathology following ischemia-reperfusion (I/R) and treatment with empagliflozin and nitric oxide modulators (H&E, × 400). (A) Control group with normal renal structure. (B) I/R group showing severe injury, including inflammation (yellow arrows), tubular dilation (green arrows), mesangial proliferation (blue arrows), hemorrhage (black arrows), and tubular degeneration (gray arrows). (C) I/R + empagliflozin: partial recovery with reduced tissue lesions. (D) I/R + empagliflozin + L-NAME: attenuated protection with persistent pathological changes. (E) I/R + empagliflozin + L-arginine: marked improvement with decreased inflammatory and degenerative alterations
.
Renal histopathology following ischemia-reperfusion (I/R) and treatment with empagliflozin and nitric oxide modulators (H&E, × 400). (A) Control group with normal renal structure. (B) I/R group showing severe injury, including inflammation (yellow arrows), tubular dilation (green arrows), mesangial proliferation (blue arrows), hemorrhage (black arrows), and tubular degeneration (gray arrows). (C) I/R + empagliflozin: partial recovery with reduced tissue lesions. (D) I/R + empagliflozin + L-NAME: attenuated protection with persistent pathological changes. (E) I/R + empagliflozin + L-arginine: marked improvement with decreased inflammatory and degenerative alterations
Discussion
The findings of the present study demonstrate that RIR induces significant oxidative stress and inflammatory responses, which contribute to structural kidney damage. Histological analysis revealed prominent pathological alterations, including hemorrhage, tubular degeneration and dilation, inflammation, and glomerular mesenchymal proliferation. These structural changes were accompanied by elevated serum levels of urea and creatinine, reflecting impaired renal function. Treatment with empagliflozin markedly attenuated these pathological changes, reduced oxidative stress, and decreased the levels of inflammatory cytokines, thereby improving renal function. These results are consistent with previous reports highlighting the renoprotective and anti-inflammatory effects of SGLT2 inhibitors in ischemic kidney injury. Interestingly, co-administration of L-NAME, a nitric oxide synthase inhibitor, with empagliflozin attenuated the drug’s protective effects. This combination led to increased oxidative stress and inflammatory markers, as well as worsened histopathological indicators, suggesting that the therapeutic benefits of empagliflozin are at least partly mediated via the NO pathway. Conversely, simultaneous administration of empagliflozin with L-arginine, a nitric oxide precursor, further enhanced renoprotection by significantly reducing oxidative stress and inflammatory cytokines and improving histological indices beyond those observed with empagliflozin alone. Collectively, these results indicate that empagliflozin exerts protective effects against ischemia-reperfusion-induced renal injury primarily through modulation of the NO signaling pathway. The combination of empagliflozin with NO stimulation may offer a synergistic approach to mitigate oxidative stress, inflammation, and structural kidney damage, thereby improving functional outcomes following renal ischemia-reperfusion.
The results of this study demonstrate that inhibition of the NO pathway by L-NAME markedly reduces the protective effects of empagliflozin, highlighting the critical role of NO signaling as a therapeutic target in ischemia-reperfusion-induced renal injury. These findings are consistent with previous studies emphasizing the critical role of NO in regulating renal hemodynamics, glomerular function, and inflammatory responses.31,32 Furthermore, co-administration of empagliflozin with L-arginine, a nitric oxide precursor, further enhanced renal function and attenuated tissue damage, suggesting a synergistic protective effect. These results underscore the potential of combination therapies in managing kidney injuries and emphasize the critical role of NO homeostasis in maintaining renal physiology. Maintaining renal physiology is crucial, and low-dose sodium nitrite, a nitric oxide donor, has been shown to protect against renal ischemia-reperfusion injury by enhancing renal oxygenation.33 Furthermore, this study confirms the renoprotective effects of empagliflozin and emphasizes the critical role of NO signaling pathways in kidney function. The results indicate that ischemia-reperfusion injury reduces NO levels in kidney tissue, which is associated with increased oxidative stress and elevated inflammatory mediators, ultimately causing structural renal damage. These findings align with previous studies reporting decreased NO bioavailability during renal ischemia-reperfusion injury.34 In the present study, tissue nitrate measurements in the second group revealed a reduction in NO levels in kidneys subjected to ischemia-reperfusion.
Moreover, numerous studies have demonstrated the renoprotective effects of empagliflozin. Clinical evidence indicates that, in addition to its safety, empagliflozin effectively reduces the risk of kidney disease progression and associated mortality in patients with chronic kidney disease.35 In chronic kidney disease, the loss of functional nephrons increases the workload on remaining nephrons, leading to elevated intraglomerular pressure, hyperfiltration, and progressive structural damage such as glomerulosclerosis and tubulointerstitial fibrosis. These injurious processes are precisely the targets of SGLT2 inhibitors, which mitigate disease progression by reducing glomerular pressure, tubular workload, and inflammation.36 Empagliflozin has been shown to increase urinary adenosine excretion and reduce hyperfiltration by promoting afferent arteriolar constriction.37 Additionally, glycosylation can trigger afferent glomerular arteriole contraction via tubuloglomerular feedback, leading to decreased glomerular pressure and filtration rate.36 Studies also indicate that empagliflozin can lower serum urea and albumin levels and mitigate both tubulointerstitial and glomerular damage.38 These findings are consistent with the results of the present study. A key distinction, however, is that our research specifically investigates the role of the NO signaling pathway. Empagliflozin preserves renal tissue structure during ischemia-reperfusion injury by significantly reducing the expression of pro-apoptotic markers such as BAX, Caspase-3, and Caspase-8.39 The elevated NO levels observed in empagliflozin-treated groups, especially when combined with L-arginine, indicate activation of the NO pathway, which likely represents a central mechanism underlying its renoprotective effects. This activation may be mediated through enhanced endothelial nitric oxide synthase (eNOS) activity and decreased oxidative stress, as reported in previous studies.40,41 Empagliflozin has been shown to enhance the bioavailability of NO by modulating and inhibiting reactive oxygen species, without altering eNOS expression or signaling.42,43 In a gentamicin-induced kidney injury model, empagliflozin increased PAX2 levels and reduced inflammatory mediators.44 PAX2, a key transcription factor, plays a critical role in kidney tissue repair and limits fibrosis.45 Additionally, the observed reductions in inflammatory cytokines and improvements in histological indices in empagliflozin-treated groups highlight its anti-inflammatory and antifibrotic effects, likely mediated through the modulation of inflammation and restoration of oxidative balance, consistent with its reported antioxidant properties.46,47 Histopathological analyses have demonstrated that empagliflozin treatment effectively mitigates cystic alterations, inflammation, tissue expansion, and overall renal damage in experimental models of chronic interstitial kidney fibrosis.48 Moreover, empagliflozin has been shown to provide renal benefits not only in diabetic patients but also in those with non-diabetic kidney disease.35,49,50 Several studies have suggested that NO plays a crucial role in protecting against kidney diseases by reducing oxidative stress and inflammatory mediators.51,52 In the present study, empagliflozin treatment improved biochemical and histological parameters in rats, and these effects were further augmented when combined with L-arginine. The observed increase in tissue nitrite levels suggests a potential involvement of NO-related signaling in mediating the renoprotective effects of empagliflozin. Increased NO bioavailability may contribute to reduced oxidative stress and inflammation; however, it should be noted that nitrite was only used as a surrogate marker, and we did not directly assess eNOS activity, phosphorylation status, or NOS isoform expression. Importantly, empagliflozin is known to exert pleiotropic effects beyond glycemic control, including AMPK activation, reduction of oxidative stress, and anti-inflammatory actions, which may also contribute to the observed protective outcomes, either independently or in concert with NO signaling.
Conclusion
The results of this study demonstrated that empagliflozin administration significantly protects against kidney damage induced by ischemia-reperfusion by reducing inflammatory cytokines and oxidative stress. This renoprotective effect of empagliflozin was markedly attenuated when co-administered with L-NAME, whereas it was enhanced with L-arginine co-administration. The observed reduction in pathological damage—including inflammation, tubular dilation, glomerular mesenchymal proliferation, hemorrhage, and tubular degeneration—suggests that the NO pathway represents a key mechanism underlying the renal protective effects of empagliflozin. The researchers recommend that future studies investigate levels of PAX2 and other relevant markers, which were not examined in this study due to its limitations. These findings provide a promising basis for the development of targeted therapies aimed at preventing or mitigating ischemia-reperfusion injury in the kidneys and underscore the need for further research into these molecular pathways and their complex interactions.
Limitations and Future Directions
Absence of direct molecular validation of NO-related pathways, such as eNOS phosphorylation or NOS isoform expression, was a limitation for this study. Due to resource constraints, we focused primarily on functional and biochemical indices (renal function markers, oxidative stress parameters, and tissue nitrite levels), which are well-established surrogate indicators of NO bioavailability in ischemia-reperfusion injury models. In addition, although the combination of empagliflozin and L-arginine demonstrated enhanced protective effects, we did not conduct a formal synergy analysis, and thus the observed outcomes should be regarded as additive rather than definitively synergistic. Another limitation is the relatively small sample size (n = 6 per group), which may reduce statistical power and generalizability. Future studies with larger cohorts and incorporation of molecular assays (e.g., western blotting, qPCR) are warranted to validate NO pathway activation and to further elucidate the mechanistic basis of empagliflozin’s renoprotective effects.
Competing Interests
The authors have no conflict of interest to declare.
Data Availability Statement
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Ethical Approval
This study was approved by the Ethics Committee of Lorestan University of Medical Sciences with the code IR.LUMS.REC.1401.256.
Acknowledgements
The research team would like to express their sincere gratitude to the esteemed Vice Chancellor for Research and Technology at Lorestan University of Medical Sciences as well as the dedicated staff of the Center for Keeping Laboratory Animals at this university.
References
- Malek M, Nematbakhsh M. Renal ischemia/reperfusion injury; from pathophysiology to treatment. J Renal InjPrev 2015; 4(2):20-7. doi: 10.12861/jrip.2015.06 [Crossref] [ Google Scholar]
- Naito H, Nojima T, Fujisaki N, Tsukahara K, Yamamoto H, Yamada T. Therapeutic strategies for ischemia reperfusion injury in emergency medicine. Acute Med Surg 2020; 7(1):e501. doi: 10.1002/ams2.501 [Crossref] [ Google Scholar]
- Frąk W, Dąbek B, Balcerczyk-Lis M, Motor J, Radzioch E, Młynarska E. Role of uremic toxins, oxidative stress, and renal fibrosis in chronic kidney disease. Antioxidants (Basel) 2024; 13(6):687. doi: 10.3390/antiox13060687 [Crossref] [ Google Scholar]
- Piko N, Bevc S, Hojs R, Ekart R. The role of oxidative stress in kidney injury. Antioxidants (Basel) 2023; 12(9):1772. doi: 10.3390/antiox12091772 [Crossref] [ Google Scholar]
- Li C, Yu Y, Zhu S, Hu Y, Ling X, Xu L. The emerging role of regulated cell death in ischemia and reperfusion-induced acute kidney injury: current evidence and future perspectives. Cell Death Discov 2024; 10(1):216. doi: 10.1038/s41420-024-01979-4 [Crossref] [ Google Scholar]
- Zhang PL, Lun M, Schworer CM, Blasick TM, Masker KK, Jones JB. Heat shock protein expression is highly sensitive to ischemia-reperfusion injury in rat kidneys. Ann Clin Lab Sci 2008; 38(1):57-64. [ Google Scholar]
- Oliveira F, Assreuy J, Sordi R. The role of nitric oxide in sepsis-associated kidney injury. Biosci Rep 2022; 42(7):BSR20220093. doi: 10.1042/bsr20220093 [Crossref] [ Google Scholar]
- Ahmad A, Dempsey SK, Daneva Z, Azam M, Li N, Li PL. Role of nitric oxide in the cardiovascular and renal systems. Int J Mol Sci 2018; 19(9):2605. doi: 10.3390/ijms19092605 [Crossref] [ Google Scholar]
- Oba S, Suzuki E, Nishimatsu H, Kumano S, Hosoda C, Homma Y. Renoprotective effect of erythropoietin in ischemia/reperfusion injury: possible roles of the Akt/endothelial nitric oxide synthase-dependent pathway. Int J Urol 2012; 19(3):248-55. doi: 10.1111/j.1442-2042.2011.02920.x [Crossref] [ Google Scholar]
- Gandhi C, Zalawadia R, Balaraman R. Nebivolol reduces experimentally induced warm renal ischemia reperfusion injury in rats. Ren Fail 2008; 30(9):921-30. doi: 10.1080/08860220802353900 [Crossref] [ Google Scholar]
- Okamoto M, Tsuchiya K, Kanematsu Y, Izawa Y, Yoshizumi M, Kagawa S. Nitrite-derived nitric oxide formation following ischemia-reperfusion injury in kidney. Am J Physiol Renal Physiol 2005; 288(1):F182-7. doi: 10.1152/ajprenal.00036.2004 [Crossref] [ Google Scholar]
- Kamenshchikov NO, Podoksenov YK, Kozlov BN, Maslov LN, Mukhomedzyanov AV, Tyo MA. The nephroprotective effect of nitric oxide during extracorporeal circulation: an experimental study. Biomedicines 2024; 12(6):1298. doi: 10.3390/biomedicines12061298 [Crossref] [ Google Scholar]
- Hu J, Spina S, Zadek F, Kamenshchikov NO, Bittner EA, Pedemonte J. Effect of nitric oxide on postoperative acute kidney injury in patients who underwent cardiopulmonary bypass: a systematic review and meta-analysis with trial sequential analysis. Ann Intensive Care 2019; 9(1):129. doi: 10.1186/s13613-019-0605-9 [Crossref] [ Google Scholar]
- Afsar B, Afsar RE. Sodium-glucose co-transporter 2 inhibitors and sarcopenia: a controversy that must be solved. Clin Nutr 2023; 42(12):2338-52. doi: 10.1016/j.clnu.2023.10.004 [Crossref] [ Google Scholar]
- Chu C, Delić D, Alber J, Feger M, Xiong Y, Luo T. Head-to-head comparison of two SGLT-2 inhibitors on AKI outcomes in a rat ischemia-reperfusion model. Biomed Pharmacother 2022; 153:113357. doi: 10.1016/j.biopha.2022.113357 [Crossref] [ Google Scholar]
- Tauber P, Sinha F, Berger RS, Gronwald W, Dettmer K, Kuhn M. Empagliflozin reduces renal hyperfiltration in response to uninephrectomy, but is not nephroprotective in UNx/DOCA/salt mouse models. Front Pharmacol 2021; 12:761855. doi: 10.3389/fphar.2021.761855 [Crossref] [ Google Scholar]
- Škrtić M, Cherney DZ. Sodium-glucose cotransporter-2 inhibition and the potential for renal protection in diabetic nephropathy. CurrOpin Nephrol Hypertens 2015; 24(1):96-103. doi: 10.1097/mnh.0000000000000084 [Crossref] [ Google Scholar]
- Wang Q, Ju F, Li J, Liu T, Zuo Y, Abbott GW. Empagliflozin protects against renal ischemia/reperfusion injury in mice. Sci Rep 2022; 12(1):19323. doi: 10.1038/s41598-022-24103-x [Crossref] [ Google Scholar]
- Yang W, Li X, He L, Zhu S, Lai S, Zhang X. Empagliflozin improves renal ischemia-reperfusion injury by reducing inflammation and enhancing mitochondrial fusion through AMPK-OPA1 pathway promotion. Cell Mol Biol Lett 2023; 28(1):42. doi: 10.1186/s11658-023-00457-6 [Crossref] [ Google Scholar]
- Juni RP, Al-Shama R, Kuster DW, van der Velden J, Hamer HM, Vervloet MG. Empagliflozin restores chronic kidney disease-induced impairment of endothelial regulation of cardiomyocyte relaxation and contraction. Kidney Int 2021; 99(5):1088-101. doi: 10.1016/j.kint.2020.12.013 [Crossref] [ Google Scholar]
- Chen S, Wang Q, Bakker D, Hu X, Zhang L, van der Made I. Empagliflozin prevents heart failure through inhibition of the NHE1-NO pathway, independent of SGLT2. Basic Res Cardiol 2024; 119(5):751-72. doi: 10.1007/s00395-024-01067-9 [Crossref] [ Google Scholar]
- Li C, Zhang J, Xue M, Li X, Han F, Liu X. SGLT2 inhibition with empagliflozin attenuates myocardial oxidative stress and fibrosis in diabetic mice heart. Cardiovasc Diabetol 2019; 18(1):15. doi: 10.1186/s12933-019-0816-2 [Crossref] [ Google Scholar]
- Gallo LA, Ward MS, Fotheringham AK, Zhuang A, Borg DJ, Flemming NB. Once daily administration of the SGLT2 inhibitor, empagliflozin, attenuates markers of renal fibrosis without improving albuminuria in diabetic db/db mice. Sci Rep 2016; 6:26428. doi: 10.1038/srep26428 [Crossref] [ Google Scholar]
- Sabbaghziarani F, Mortezaee K, Hassanzadeh G, Noori-Mugahi SM. Effects of L-arginine and L-NAME on duodenal histologic parameters in female Wistar rats. Anat Sci J 2014; 11(4):163-8. [ Google Scholar]
- Ebadi B, Mehdizadeh M, Nahavandi A, Shariati T, Delaviz H. The effect of L-arginine on the brain tissue of stressed rats. Basic Clin Neurosci 2010; 1(2):33-6. [ Google Scholar]
- Mohmoodnia L, Koushki S, Moruzzi M, Papi S, Mohammadrezaei Khorramabadi R, Farzan B. Protective effect of aliskiren against renal ischemia reperfusion via antioxidant property and nitric oxide signaling pathway. ImmunopatholPersa 2019; 5(1):e10. doi: 10.15171/ipp.2019.10 [Crossref] [ Google Scholar]
- Amani Tirani S, Pezeshki Z, Nematbakhsh M, Nasri H, Talebi A. Effect of L-arginine and L-NAME on kidney tissue damage in rats after 24 h of bilateral ureteral obstruction. Int J Prev Med 2015; 6:60. doi: 10.4103/2008-7802.160339 [Crossref] [ Google Scholar]
- Hasanvand A, Pirzadroozbahani N, Ahmadizar F, Kharazmkia A, Mir S, Amanolahi Baharvand P. Evaluation of the antioxidant effects of zolpidem in the rat model of cisplatin-induced nephrotoxicity. J Renal InjPrev 2018; 7(4):235-9. doi: 10.15171/jrip.2018.54 [Crossref] [ Google Scholar]
- Lepoivre M, Chenais B, Yapo A, Lemaire G, Thelander L, Tenu JP. Alterations of ribonucleotide reductase activity following induction of the nitrite-generating pathway in adenocarcinoma cells. J Biol Chem 1990; 265(24):14143-9. [ Google Scholar]
- Nogueira GB, Punaro GR, Oliveira CS, Maciel FR, Fernandes TO, Lima DY. N-acetylcysteine protects against diabetic nephropathy through control of oxidative and nitrosative stress by recovery of nitric oxide in rats. Nitric Oxide 2018; 78:22-31. doi: 10.1016/j.niox.2018.05.003 [Crossref] [ Google Scholar]
- Ragy MM, Aziz NM. Prevention of renal ischemia/perfusion-induced renal and hepatic injury in adult male albino rats by oxytocin: role of nitric oxide. J Basic Clin PhysiolPharmacol 2017; 28(6):615-21. doi: 10.1515/jbcpp-2016-0197 [Crossref] [ Google Scholar]
- Tripatara P, Patel NS, Webb A, Rathod K, Lecomte FM, Mazzon E. Nitrite-derived nitric oxide protects the rat kidney against ischemia/reperfusion injury in vivo: role for xanthine oxidoreductase. J Am Soc Nephrol 2007; 18(2):570-80. doi: 10.1681/asn.2006050450 [Crossref] [ Google Scholar]
- Cantow K, Flemming B, Ladwig-Wiegard M, Persson PB, Seeliger E. Low dose nitrite improves reoxygenation following renal ischemia in rats. Sci Rep 2017; 7(1):14597. doi: 10.1038/s41598-017-15058-5 [Crossref] [ Google Scholar]
- Yang T, Zhang XM, Tarnawski L, Peleli M, Zhuge Z, Terrando N. Dietary nitrate attenuates renal ischemia-reperfusion injuries by modulation of immune responses and reduction of oxidative stress. Redox Biol 2017; 13:320-30. doi: 10.1016/j.redox.2017.06.002 [Crossref] [ Google Scholar]
- Herrington WG, Staplin N, Wanner C, Green JB, Hauske SJ, Emberson JR. Empagliflozin in patients with chronic kidney disease. N Engl J Med 2023; 388(2):117-27. doi: 10.1056/NEJMoa2204233 [Crossref] [ Google Scholar]
- Chen X, Hocher CF, Shen L, Krämer BK, Hocher B. Reno- and cardioprotective molecular mechanisms of SGLT2 inhibitors beyond glycemic control: from bedside to bench. Am J Physiol Cell Physiol 2023; 325(3):C661-c81. doi: 10.1152/ajpcell.00177.2023 [Crossref] [ Google Scholar]
- Kidokoro K, Cherney DZ, Bozovic A, Nagasu H, Satoh M, Kanda E. Evaluation of glomerular hemodynamic function by empagliflozin in diabetic mice using in vivo imaging. Circulation 2019; 140(4):303-15. doi: 10.1161/circulationaha.118.037418 [Crossref] [ Google Scholar]
- Ala M, Fallahpour Khoshdel MR, Dehpour AR. Empagliflozin enhances autophagy, mitochondrial biogenesis, and antioxidant defense and ameliorates renal ischemia/reperfusion in nondiabetic rats. Oxid Med Cell Longev 2022; 2022:1197061. doi: 10.1155/2022/1197061 [Crossref] [ Google Scholar]
- Cheng J, Zhang X, Zheng Q, Shi S, Wang J. Empagliflozin-loaded nanomicelles responsive to reactive oxygen species for renal ischemia/reperfusion injury protection. Open Chem 2024; 22(1):20240015. doi: 10.1515/chem-2024-0015 [Crossref] [ Google Scholar]
- Santos-Gallego CG, Requena-Ibanez JA, San Antonio R, Garcia-Ropero A, Ishikawa K, Watanabe S. Empagliflozin ameliorates diastolic dysfunction and left ventricular fibrosis/stiffness in nondiabetic heart failure: a multimodality study. JACC Cardiovasc Imaging 2021; 14(2):393-407. doi: 10.1016/j.jcmg.2020.07.042 [Crossref] [ Google Scholar]
- Campeau MA, Leask RL. Empagliflozin mitigates endothelial inflammation and attenuates endoplasmic reticulum stress signaling caused by sustained glycocalyx disruption. Sci Rep 2022; 12(1):12681. doi: 10.1038/s41598-022-16763-6 [Crossref] [ Google Scholar]
- Uthman L, Homayr A, Juni RP, Spin EL, Kerindongo R, Boomsma M. Empagliflozin and dapagliflozin reduce ROS generation and restore NO bioavailability in tumor necrosis factor α-stimulated human coronary arterial endothelial cells. Cell PhysiolBiochem 2019; 53(5):865-86. doi: 10.33594/000000178 [Crossref] [ Google Scholar]
- Li X, Wang M, Kalina JO, Preckel B, Hollmann MW, Albrecht M. Empagliflozin prevents oxidative stress in human coronary artery endothelial cells via the NHE/PKC/NOX axis. Redox Biol 2024; 69:102979. doi: 10.1016/j.redox.2023.102979 [Crossref] [ Google Scholar]
- Botros SR, Matouk AI, Anter A, Khalifa MM, Heeba GH. Protective effect of empagliflozin on gentamicin-induced acute renal injury via regulation of SIRT1/NF-κB signaling pathway. Environ ToxicolPharmacol 2022; 94:103907. doi: 10.1016/j.etap.2022.103907 [Crossref] [ Google Scholar]
- Sako K, Furuichi K, Makiishi S, Yamamura Y, Okumura T, Le HT. Cyclin-dependent kinase 4-related tubular epithelial cell proliferation is regulated by paired box gene 2 in kidney ischemia-reperfusion injury. Kidney Int 2022; 102(1):45-57. doi: 10.1016/j.kint.2022.03.022 [Crossref] [ Google Scholar]
- Das NA, Carpenter AJ, Belenchia A, Aroor AR, Noda M, Siebenlist U. Empagliflozin reduces high glucose-induced oxidative stress and miR-21-dependent TRAF3IP2 induction and RECK suppression, and inhibits human renal proximal tubular epithelial cell migration and epithelial-to-mesenchymal transition. Cell Signal 2020; 68:109506. doi: 10.1016/j.cellsig.2019.109506 [Crossref] [ Google Scholar]
- Badreldin H, El-Karef A, Ibrahim T, Elshal M. Targeting Nrf2/HO-1 and NF-κB/TNF-α signaling pathways with empagliflozin protects against atrial fibrillation-induced acute kidney injury in rats. Toxicology 2024; 506:153879. doi: 10.1016/j.tox.2024.153879 [Crossref] [ Google Scholar]
- Abbas NA, El Salem A, Awad MM. Empagliflozin, SGLT2 inhibitor, attenuates renal fibrosis in rats exposed to unilateral ureteric obstruction: potential role of klotho expression. NaunynSchmiedebergs Arch Pharmacol 2018; 391(12):1347-60. doi: 10.1007/s00210-018-1544-y [Crossref] [ Google Scholar]
- Zannad F, Ferreira JP, Pocock SJ, Zeller C, Anker SD, Butler J. Cardiac and kidney benefits of empagliflozin in heart failure across the spectrum of kidney function: insights from EMPEROR-Reduced. Circulation 2021; 143(4):310-21. doi: 10.1161/circulationaha.120.051685 [Crossref] [ Google Scholar]
- Fernandez-Fernandez B, Sarafidis P, Kanbay M, Navarro-González JF, Soler MJ, Górriz JL. SGLT2 inhibitors for non-diabetic kidney disease: drugs to treat CKD that also improve glycaemia. Clin Kidney J 2020; 13(5):728-33. doi: 10.1093/ckj/sfaa198 [Crossref] [ Google Scholar]
- Nascimento M, Punaro GR, Serralha RS, Lima DY, Mouro MG, Oliveira LCG. Inhibition of the P2X7 receptor improves renal function via renin-angiotensin system and nitric oxide on diabetic nephropathy in rats. Life Sci 2020; 251:117640. doi: 10.1016/j.lfs.2020.117640 [Crossref] [ Google Scholar]
- Gholampour F, Khangah L, Vatanparast J, Karbalaei-Heidari HR, Owji SM, Bahaoddini A. The role of nitric oxide in the protective action of remote ischemic per-conditioning against ischemia/reperfusion-induced acute renal failure in rat. Iran J Basic Med Sci 2018; 21(6):600-6. doi: 10.22038/ijbms.2018.25810.6354 [Crossref] [ Google Scholar]